Full mouth rehabilitation using orthodontic treatment and implants in patient with collapsed occlusion: A case report
- Affiliations
-
- 1Department of Prosthodontics, Seoul National University School of Dentistry, Seoul, Republic of Korea. young21c@snu.ac.kr
- KMID: 2461152
- DOI: http://doi.org/10.4047/jkap.2019.57.4.439
Abstract
- The distance between the natural teeth and the implants is an important factor in preserving the periodontal tissues and esthetics. And abnormal positional displacement and tilting of the teeth during restorative procedure may require intentional root canal treatment and may affect masticatory function. This report is to present a successful full mouth rehabilitation of a patient with uneven dentition and collapsed occlusion using orthodontic and implant treatment. The patient had no symptoms or discomfort of temporomandibular joint disorder such as pain or sound. The orthodontic treatment was continued until implant provisional prosthesis delivery. And the vertical height of occlusion was elevated 2mm on anterior basis for anterior teeth protection and esthetics. After the orthodontic treatment, the implant abutments and natural teeth were finally restored with porcelain-fused-to-metal crowns and bridges. Satisfactory function and esthetic outcomes are observed after 6months of follow up.
Keyword
MeSH Terms
Figure
-
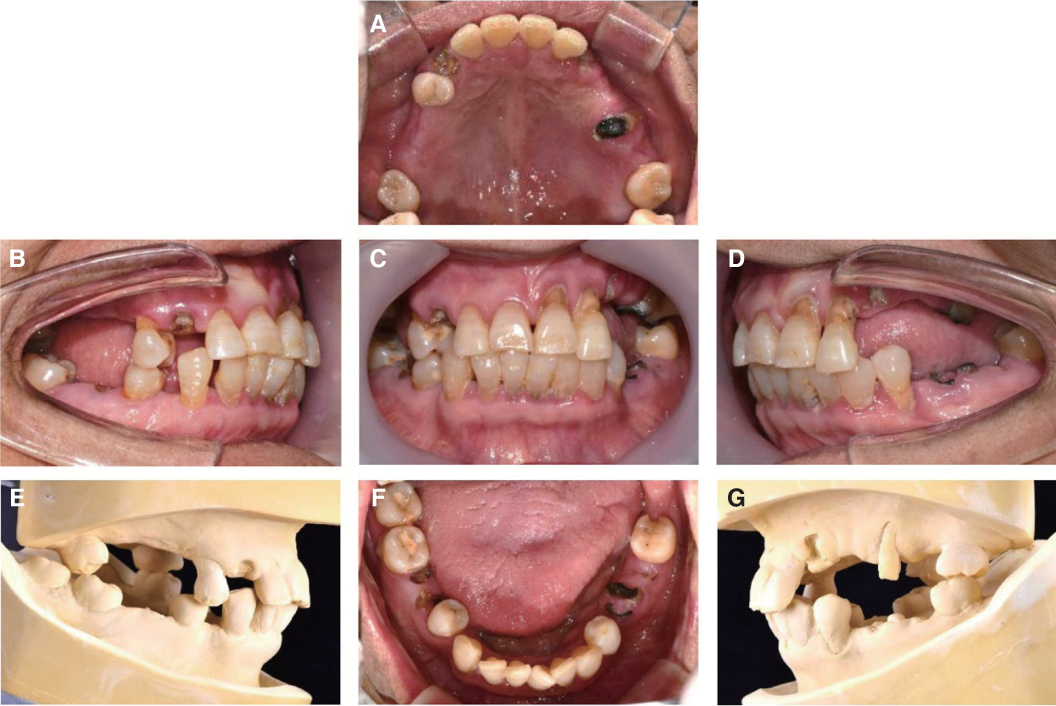
Fig. 1 Intraoral photograph & diagnostic model before treatment. (A) Maxillary, (B) Right, (C) Frontal, (D) Left, (E) Right of the diagnostic model, (F) Mandibular, (G) Left of the diagnostic model.

Fig. 2 Tooth examination. (A) Examination chart of maxilla, (B) Intraoral radiographs, (C) Examination chart of mandible.

Fig. 3 Radiographic evaluation before treatment. (A) Panoramic radiograph, (B) TMJ panoramic view.

Fig. 4 Orthodontic treatment. (A) Frontal view with clear orthodontic aligner (4th step), (B) 1st RP model, (C) Final RP model.
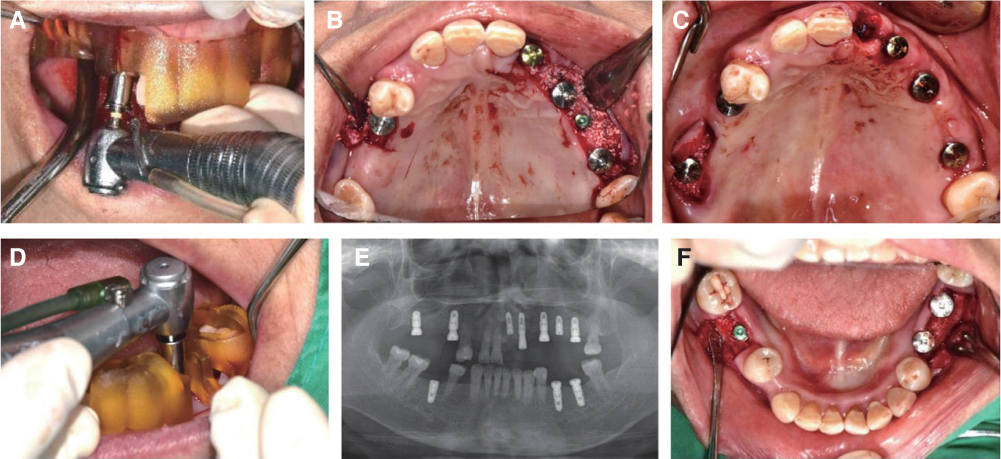
Fig. 5 Implant installation with surgical guide. (A, D) CT guided implant surgery with surgical guide, (B) After primary surgery of Maxilla, (C, F) After implant 1st surgery, (E) Panoramic radiograph after implant surgery.
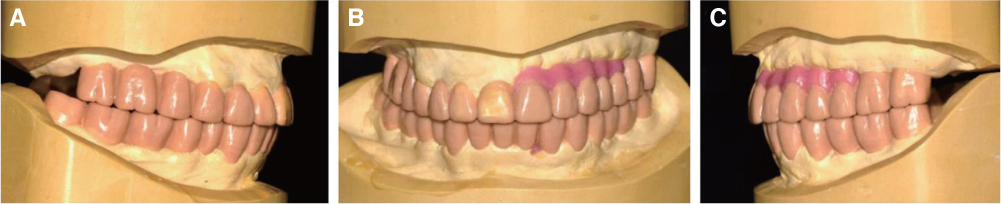
Fig. 6 Diagnostic wax up model. (A) Right, (B) Frontal, (C) Left.
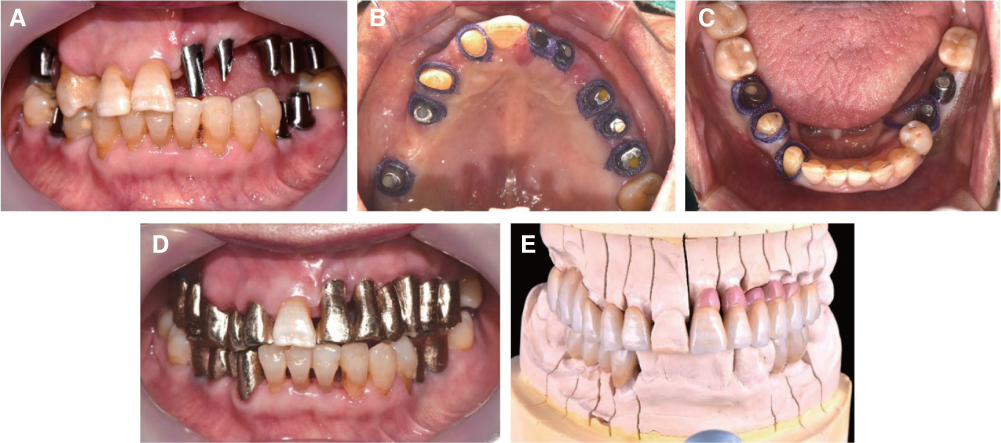
Fig. 7 Prosthetic procedure. (A) Custom abutment delivery, (B, C) Abutment level impression (maxillary, mandibular), (D) Metal coping try-in, (E) Porcelain build up and glazing.

Fig. 8 Definitive prosthesis. (A) Upper, (B) Right, (C) Frontal, (D) Left, (E) Panoramic photograph after delivery, (F) Lower, (G) TMJ panoramic view after delivery.
Reference
-
1. Cao T, Xu L, Shi J, Zhou Y. Combined orthodontic-periodontal treatment in periodontal patients with anteriorly displaced incisors. Am J Orthod Dentofacial Orthop. 2015; 148:805–813.
Article2. Alfuriji S, Alhazmi N, Alhamlan N, Al-Ehaideb A, Alruwaithi M, Alkatheeri N, Geevarghese A. The effect of orthodontic therapy on periodontal health: a review of the literature. Int J Dent. 2014; 2014:585048.
Article3. Greene CS, Galang-Boquiren MTS, Bartilotta BY. Orthodontics and the temporomandibular joint: What orthodontic providers need to know. Quintessence Int. 2017; 48:799–808.4. Willis FM. Features of the face involved in full denture prosthesis. Dental Cosmos. 1935; 77:851–854.5. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984; 52:467–474.
Article6. Dawson PE. Evaluation, diagnosis, and treatment of occlusal problem. Saint Louis: The C. V. Mosby Co.;1974.7. Schneider D, Schober F, Grohmann P, Hammerle CH, Jung RE. In-vitro evaluation of the tolerance of surgical instruments in templates for computer-assisted guided implantology produced by 3-D printing. Clin Oral Implants Res. 2015; 26:320–325.
Article8. Ormianer Z, Gross M. A 2-year follow-up of mandibular posture following an increase in occlusal vertical dimension beyond the clinical rest position with fixed restorations. J Oral Rehabil. 1998; 25:877–883.
Article9. Ormianer Z, Palty A. Altered vertical dimension of occlusion: a comparative retrospective pilot study of tooth- and implant-supported restorations. Int J Oral Maxillofac Implants. 2009; 24:497–501.10. Korean Association of Orthodontists: Publishing committee of a white paper on malocclusion. Report of measurement results of lateral cephalogram in Korean adults with normal occlusion. Korean Association of Orthodontists;1997.11. Krishnan V, Davidovitch Z. The effect of drugs on orthodontic tooth movement. Orthod Craniofac Res. 2006; 9:163–171.
Article12. Jiang Q, Li J, Mei L, Du J, Levrini L, Abbate GM, Li H. Periodontal health during orthodontic treatment with clear aligners and fixed appliances: A meta-analysis. J Am Dent Assoc. 2018; 149:712–720.e12.13. Dawson PE. Functional occlusion from TMJ to smile design. Mosby Elsevier;2007.14. Gopi Chander N, Venkat R. An appraisal on increasing the occlusal vertical dimension in full occlusal rehabilitation and its outcome. J Indian Prosthodont Soc. 2011; 11:77–81.
Article15. Abduo J, Lyons K. Clinical considerations for increasing occlusal vertical dimension: a review. Aust Dent J. 2012; 57:2–10.
Article16. Marcotte GR, West DW, Baar K. The molecular basis for load-induced skeletal muscle hypertrophy. Calcif Tissue Int. 2015; 96:196–210.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full mouth rehabilitation using removable prosthesis of patient with unstable mandible movements: A case report
- Full-mouth rehabilitation of a patient with loss of posterior support and collapsed occlusion utilizing dental CAD-CAM system
- Full mouth rehabilitation of deep bite patient with segmental osteotomy and orthodontic treatment
- A case of full mouth rehabilitation with orthodontic treatment in patient with extensive tooth erosion and wear using monolithic zirconia prostheses
- A case of full mouth rehabilitation in patient with loss of vertical dimension and deep bite due to tooth wear
