Bevacizumab Plus Erlotinib Combination Therapy for Advanced Hereditary Leiomyomatosis and Renal Cell Carcinoma-Associated Renal Cell Carcinoma: A Multicenter Retrospective Analysis in Korean Patients
- Affiliations
-
- 1Division of Medical Oncology, Department of Internal Medicine, Seoul National University Hospital, Seoul, Korea.
- 2Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 3Division of Hematology and Medical Oncology, Dongguk University Ilsan Hospital, Goyang, Korea.
- 4Department of Internal Medicine, Konyang University Hospital, Daejeon, Korea.
- 5Department of Laboratory Medicine, Gachon University Gil Medical Center, Incheon, Korea.
- 6Division of Medical Oncology, Department of Internal Medicine, Gachon University Gil Medical Center, Incheon, Korea. ingni79@gilhospital.com
- KMID: 2460603
- DOI: http://doi.org/10.4143/crt.2019.086
Abstract
- PURPOSE
Hereditary leiomyomatosis and renal cell carcinoma (HLRCC) is a rare genetic syndrome resulting from germline mutations in fumarate hydratase. The combination of bevacizumab plus erlotinib showed promising interim results for HLRCC-associated RCC. Based on these results, we analyzed the outcome of bevacizumab plus erlotinib in Korean patients with HLRCC-associated RCC.
MATERIALS AND METHODS
We retrospectively reviewed the efficacy and safety of bevacizumab plus erlotinib in patients with HLRCC-associated RCC who were confirmed to have germline mutations in fumarate hydratase. The primary endpoint was the objective response rate (ORR), while the secondary endpoints were progression-free survival (PFS) and overall survival (OS). RESULT: We identified 10 patients with advanced HLRCC-associated RCC who received bevacizumab plus erlotinib. Median age at diagnosis was 41 years, and five of the patients had received the combination as first- or second-line treatments. The ORR was 50% and the median PFS and OS were 13.3 and 14.1 months, respectively. Most adverse events were predictable and manageable by conventional measures, except for one instance where a patient died of gastrointestinal bleeding.
CONCLUSION
This is the first real-world outcome of the treatment of advanced HLRCC-associated RCC. Bevacizumab plus erlotinib therapy showed promising activity with moderate toxicity. We should be increasingly aware of HLRCC-associated RCC and bevacizumab plus erlotinib should be a first-line treatment for this condition, unless other promising data are published.
Keyword
MeSH Terms
Figure
-
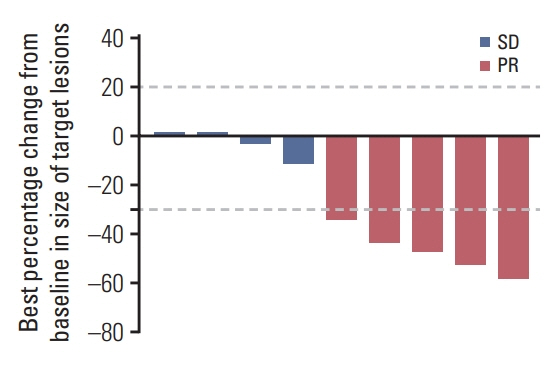
Fig. 1. Waterfall plots depicting change from baseline in sum of diameters for target lesions in patients with hereditary leiomyomatosis and renal cell carcinoma–associated renal cell carcinoma treated with bevacizumab plus erlotinib (n=9). SD, stable disease; PR, partial response.

Fig. 2. Kaplan-Meier curve for progression-free survival (PFS) and overall survival (OS) in patient with hereditary leiomyomatosis and renal cell carcinoma–associated renal cell carcinoma treated with bevacizumab plus erlotinib.
Cited by 3 articles
-
Genotypic and Phenotypic Characteristics of Hereditary Leiomyomatosis and Renal Cell Cancer Syndrome in Korean Patients
Ja Young Seo, Jeong-Yeal Ahn, Bhumsuk Keam, Miso Kim, Shinkyo Yoon, Jae Lyun Lee, Kwonoh Park, Inkeun Park
Ann Lab Med. 2021;41(2):207-213. doi: 10.3343/alm.2021.41.2.207.Clinical practice recommendations for the use of next-generation sequencing in patients with solid cancer: a joint report from KSMO and KSP
Miso Kim, Hyo Sup Shim, Sheehyun Kim, In Hee Lee, Jihun Kim, Shinkyo Yoon, Hyung-Don Kim, Inkeun Park, Jae Ho Jeong, Changhoon Yoo, Jaekyung Cheon, In-Ho Kim, Jieun Lee, Sook Hee Hong, Sehhoon Park, Hyun Ae Jung, Jin Won Kim, Han Jo Kim, Yongjun Cha, Sun Min Lim, Han Sang Kim, Choong-Kun Lee, Jee Hung Kim, Sang Hoon Chun, Jina Yun, So Yeon Park, Hye Seung Lee, Yong Mee Cho, Soo Jeong Nam, Kiyong Na, Sun Och Yoon, Ahwon Lee, Kee-Taek Jang, Hongseok Yun, Sungyoung Lee, Jee Hyun Kim, Wan-Seop Kim
J Pathol Transl Med. 2024;58(4):147-164. doi: 10.4132/jptm.2023.11.01.Clinical Practice Recommendations for the Use of Next-Generation Sequencing in Patients with Solid Cancer: A Joint Report from KSMO and KSP
Miso Kim, Hyo Sup Shim, Sheehyun Kim, In Hee Lee, Jihun Kim, Shinkyo Yoon, Hyung-Don Kim, Inkeun Park, Jae Ho Jeong, Changhoon Yoo, Jaekyung Cheon, In-Ho Kim, Jieun Lee, Sook Hee Hong, Sehhoon Park, Hyun Ae Jung, Jin Won Kim, Han Jo Kim, Yongjun Cha, Sun Min Lim, Han Sang Kim, Choong-kun Lee, Jee Hung Kim, Sang Hoon Chun, Jina Yun, So Yeon Park, Hye Seung Lee, Yong Mee Cho, Soo Jeong Nam, Kiyong Na, Sun Och Yoon, Ahwon Lee, Kee-Taek Jang, Hongseok Yun, Sungyoung Lee, Jee Hyun Kim, Wan-Seop Kim
Cancer Res Treat. 2024;56(3):721-742. doi: 10.4143/crt.2023.1043.
Reference
-
References
1. Tomlinson IP, Alam NA, Rowan AJ, Barclay E, Jaeger EE, Kelsell D, et al. Germline mutations in FH predispose to dominantly inherited uterine fibroids, skin leiomyomata and papillary renal cell cancer. Nat Genet. 2002; 30:406–10.
Article2. Linehan WM, Rouault TA. Molecular pathways: Fumarate hydratase-deficient kidney cancer: targeting the Warburg effect in cancer. Clin Cancer Res. 2013; 19:3345–52.3. Lehtonen HJ. Hereditary leiomyomatosis and renal cell cancer: update on clinical and molecular characteristics. Fam Cancer. 2011; 10:397–411.
Article4. Moch H, Cubilla AL, Humphrey PA, Reuter VE, Ulbright TM. The 2016 WHO classification of tumours of the urinary system and male genital organs-part A: renal, penile, and testicular tumours. Eur Urol. 2016; 70:93–105.
Article5. Srinivasan R, Ricketts CJ, Sourbier C, Linehan WM. New strategies in renal cell carcinoma: targeting the genetic and metabolic basis of disease. Clin Cancer Res. 2015; 21:10–7.
Article6. Yang L, Xie M, Yang M, Yu Y, Zhu S, Hou W, et al. PKM2 regulates the Warburg effect and promotes HMGB1 release in sepsis. Nat Commun. 2014; 5:4436.
Article7. De Rosa V, Iommelli F, Monti M, Fonti R, Votta G, Stoppelli MP, et al. Reversal of Warburg effect and reactivation of oxidative phosphorylation by differential inhibition of EGFR signaling pathways in non-small cell lung cancer. Clin Cancer Res. 2015; 21:5110–20.
Article8. Srinivasan R, Su D, Stamatakis L, Siddiqui MM, Singer E, Shuch B, et al. 5 Mechanism based targeted therapy for hereditary leiomyomatosis and renal cell cancer (HLRCC) and sporadic papillary renal cell carcinoma: interim results from a phase 2 study of bevacizumab and erlotinib. Eur J Cancer. 2014; 50(Suppl 6):8.
Article9. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology. Kidney cancer (ver 2. 2019) [Internet]. National Comprehensive Cancer Network;2019. Available from: https://www.nccn.org/professionals/physician_gls/pdf/kidney.pdf.10. Grubb RL 3rd, Franks ME, Toro J, Middelton L, Choyke L, Fowler S, et al. Hereditary leiomyomatosis and renal cell cancer: a syndrome associated with an aggressive form of inherited renal cancer. J Urol. 2007; 177:2074–9.
Article11. Alrashdi I, Levine S, Paterson J, Saxena R, Patel SR, Depani S, et al. Hereditary leiomyomatosis and renal cell carcinoma: very early diagnosis of renal cancer in a paediatric patient. Fam Cancer. 2010; 9:239–43.
Article12. Merino MJ, Torres-Cabala C, Pinto P, Linehan WM. The morphologic spectrum of kidney tumors in hereditary leiomyomatosis and renal cell carcinoma (HLRCC) syndrome. Am J Surg Pathol. 2007; 31:1578–85.
Article13. Menko FH, Maher ER, Schmidt LS, Middelton LA, Aittomaki K, Tomlinson I, et al. Hereditary leiomyomatosis and renal cell cancer (HLRCC): renal cancer risk, surveillance and treatment. Fam Cancer. 2014; 13:637–44.
Article14. Dienstmann R, Brana I, Rodon J, Tabernero J. Toxicity as a biomarker of efficacy of molecular targeted therapies: focus on EGFR and VEGF inhibiting anticancer drugs. Oncologist. 2011; 16:1729–40.
Article15. Sorich MJ, Rowland A, Kichenadasse G, Woodman RJ, Mangoni AA. Risk factors of proteinuria in renal cell carcinoma patients treated with VEGF inhibitors: a secondary analysis of pooled clinical trial data. Br J Cancer. 2016; 114:1313–7.
Article16. Lattouf JB, Pautler SE, Reaume MN, Kim RH, Care M, Green J, et al. Structured assessment and followup for patients with hereditary kidney tumour syndromes. Can Urol Assoc J. 2016; 10:E214–22.
Article
