Hepatic Involvement of Histiocytic Sarcoma: CT and MRI Findings
- Affiliations
-
- 1Department of Radiology, Graduate School of Medicine, University of Tokyo, Tokyo 113-8654, Japan.
- 2Department of Radiology, Institute of Medical Science, University of Tokyo, Tokyo 108-8639, Japan. kiryu-tky@umin.ac.jp
- 3Department of Pathology, Institute of Medical Science, University of Tokyo, Tokyo 108-8639, Japan.
- 4Department of Hematology and Oncology, Institute of Medical Science, University of Tokyo, Tokyo 108-8639, Japan.
- 5Department of Gastroenterology, Japanese Red Cross Medical Center, Tokyo 150-8935, Japan.
- 6Advanced Medical Science, Institute of Medical Science, University of Tokyo, Tokyo 108-8639, Japan.
- KMID: 2458068
- DOI: http://doi.org/10.3348/kjr.2016.17.5.758
Abstract
- Histiocytic sarcoma in the liver is an extremely rare hematological malignancy. Herein, we reported the case of a 68-year-old woman who presented with characteristic wedge-shaped abnormality bounded by hepatic veins on computed tomography and magnetic resonance imaging of the liver. In the wedge-shaped area, decreased portal flow and the deposition of iron were observed. These imaging findings are consistent with intrasinusoidal tumor cell infiltration. A liver biopsy was performed, and histiocytic sarcoma was confirmed histopathologically.
MeSH Terms
Figure
-
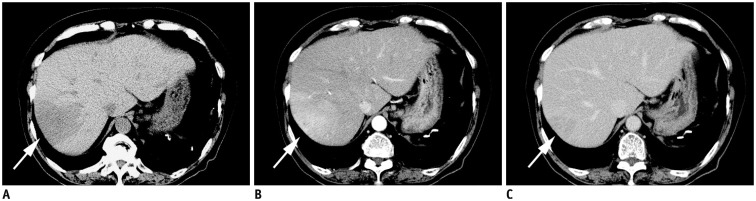
Fig. 1 Dynamic study CT.A. Precontrast CT shows slightly hypoattenuating mass in right lobe of liver (arrow). B. On arterial phase, faint enhancement is seen in this area (arrow). C. Most of area was enhanced as normal liver parenchyma on delayed phase (arrow).
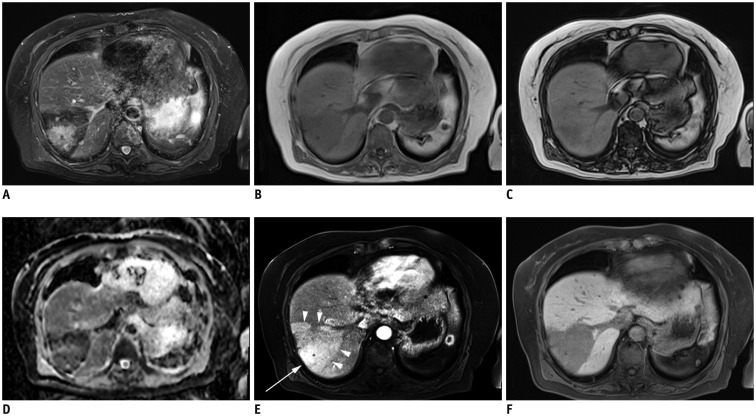
Fig. 2 MR images of liver.A. Ill-defined hyperintense signal area was found in wedge-shaped dark signal intensity area on fat-suppressed T2WI. B-D. Signal intensity was lower on in-phase images (B) than on out-of-phase images (C) in area corresponding to ill-defined hyperintense signal on fat-suppressed T2WI. Surrounding area showed low signal due to iron deposition (D). On ADC map, restricted diffusion was absent. E. After Gd-EOB-DTPA injection, enhancement (arrow) was surrounded by wedge-shaped faint enhancement (arrowheads) on arterial phase. F. Well-defined wedge-shaped decrease in Gd-EOB-DTPA was found on hepatobiliary phase. ADC = apparent diffusion coefficient, Gd-EOB-DTPA = gadolinium-ethoxybenzyl-diethylenetriamine pentaacetic acid, T2WI = T2-weighted image
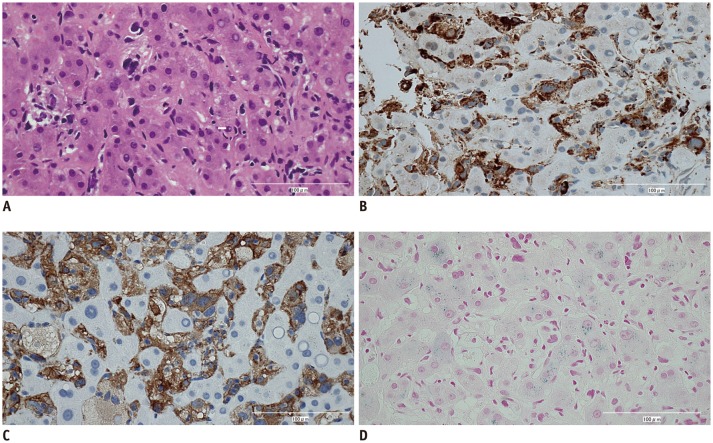
Fig. 3 Hematoxylin and eosin and immunohistochemically stained sections from liver tumor (x 200).Tumor cells showed large pleomorphic nuclei (A) and positive staining for CD68 (B) and CD163 (C). Hepatocytes were positive for iron (D).
Reference
-
1. Grogan TM, Pileri SA, Chan JKC, Weiss LM, Fletcher CDM. Histiocytic sarcoma. In : Swerdlow SH, Campo E, Harris NL, Jaffe ES, Pileri S, Stein H, editors. World Health Organization classification of tumours pathology and genetics of tumours of haematopoietic and lymphoid tissues. 4th ed. Lyon: IARC Press;2008. p. 356–357.2. Hornick JL, Jaffe ES, Fletcher CD. Extranodal histiocytic sarcoma: clinicopathologic analysis of 14 cases of a rare epithelioid malignancy. Am J Surg Pathol. 2004; 28:1133–1144. PMID: 15316312.3. Kimura H, Nasu K, Sakai C, Shiga Y, Miyamoto E, Shintaku M, et al. Histiocytic sarcoma of the spleen associated with hypoalbuminemia, hypo gamma-globulinemia and thrombocytopenia as a possibly unique clinical entity--report of three cases. Leuk Lymphoma. 1998; 31:217–224. PMID: 9720731.4. Porter DW, Gupte GL, Brown RM, Spray C, English MW, deVille DeGoyet J, et al. Histiocytic sarcoma with interdigitating dendritic cell differentiation. J Pediatr Hematol Oncol. 2004; 26:827–830. PMID: 15591905.5. Kobayashi S, Kimura F, Hama Y, Ogura K, Torikai H, Kobayashi A, et al. Histiocytic sarcoma of the spleen: case report of asymptomatic onset of thrombocytopenia and complex imaging features. Int J Hematol. 2008; 87:83–87. PMID: 18224419.
Article6. Audouin J, Vercelli-Retta J, Le Tourneau A, Adida C, Camilleri-Broët S, Molina T, et al. Primary histiocytic sarcoma of the spleen associated with erythrophagocytic histiocytosis. Pathol Res Pract. 2003; 199:107–112. PMID: 12747473.
Article7. Yamamoto S, Tsukamoto T, Kanazawa A, Shimizu S, Morimura K, Toyokawa T, et al. Laparoscopic splenectomy for histiocytic sarcoma of the spleen. World J Gastrointest Surg. 2013; 5:129–134. PMID: 23717746.
Article8. Oka K, Nakamine H, Maeda K, Yamakawa M, Imai H, Tada K, et al. Primary histiocytic sarcoma of the spleen associated with hemophagocytosis. Int J Hematol. 2008; 87:405–409. PMID: 18327679.
Article9. Shang SS, Furlan A, Almusa O, Ahmed-Amr HM, Bae KT. Regional presentation of hepatic diseases: CT and MR imaging findings of differential diagnosis. Acta Radiol. 2010; 51:832–841. PMID: 20812886.
Article10. Lupescu IG, Grasu M, Capsa R, Pitrop A, Georgescu SA. Hepatic perfusion disorders: computer-tomographic and magnetic resonance imaging. J Gastrointestin Liver Dis. 2006; 15:273–279. PMID: 17013453.11. Bayraktar UD, Seren S, Bayraktar Y. Hepatic venous outflow obstruction: three similar syndromes. World J Gastroenterol. 2007; 13:1912–1927. PMID: 17461490.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Hepatic Kaposi Sarcoma after Kidney Transplantation: A Case Report
- Histiocytic Sarcoma of Rectum: A Case Report
- Histiocytic Sarcoma of the Cervical Spinal Cord with Secondary Involvement of the Skin
- Roentgenological findings of histiocytic medullary reticulosis in the lung
- Descriptive Analysis of Histiocytic and Dendritic Cell Neoplasms: A Single-Institution Experience
