The Effect of Uncinate Process Resection on Subsidence Following Anterior Cervical Discectomy and Fusion
- Affiliations
-
- 1Department of Neurosurgery, Pusan National University Yangsan Hospital, Yangsan, Korea. md6576@naver.com
- 2Research Institute for Convergence of Biomedical Science and Technology, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 3Department of Neurosurgery, Pusan National University School of Medicine, Yangsan, Korea.
- KMID: 2457962
- DOI: http://doi.org/10.3340/jkns.2017.0202.014
Abstract
OBJECTIVE
Subsidence is a frequent complication of anterior cervical discectomy and fusion. Postoperative segmental micro-motion, thought to be a causative factor of subsidence, has been speculated to increase with uncinate process resection area (UPR). To evaluate the effect of UPR on micro-motion, we designed a method to measure UPR area based on pre- and postoperative computed tomography images and analyzed the relationship between UPR and subsidence as a proxy of micro-motion.
METHODS
We retrospectively collected clinical and radiological data from January 2011 to June 2016. A total of 38 patients (53 segments) were included. All procedures included bilateral UPR and anterior plate fixation. UPR area was evaluated with reformatted coronal computer tomography images. To reduce level-related bias, we converted UPR area to the proportion of UPR to the pre-operative UP area (pUPR).
RESULTS
Subsidence occurred in 18 segments (34%) and positively correlated with right-side pUPR, left-side pUPR, and the sum of bilateral pUPR (sum pUPR) (R=0.310, 301, 364; p=0.024, 0.029, 0.007, respectively). Multiple linear regression analysis revealed that subsidence could be estimated with the following formula: subsidence=1.522+2.7×sum pUPR (R2=0.133, p=0.007). Receiver-operating characteristic analysis determined that sum pUPR≥0.38 could serve as a threshold for significantly increased risk of subsidence (p=0.005, area under curve=0.737, sensitivity=94%, specificity=51%). This threshold was confirmed by logistic regression analysis for subsidence (p=0.009, odds ratio=8.471).
CONCLUSION
The UPR measurement method confirmed that UPR was correlated with subsidence. Particularly when the sum of pUPR is ≥38%, the possibility of subsidence increased.
MeSH Terms
Figure
-
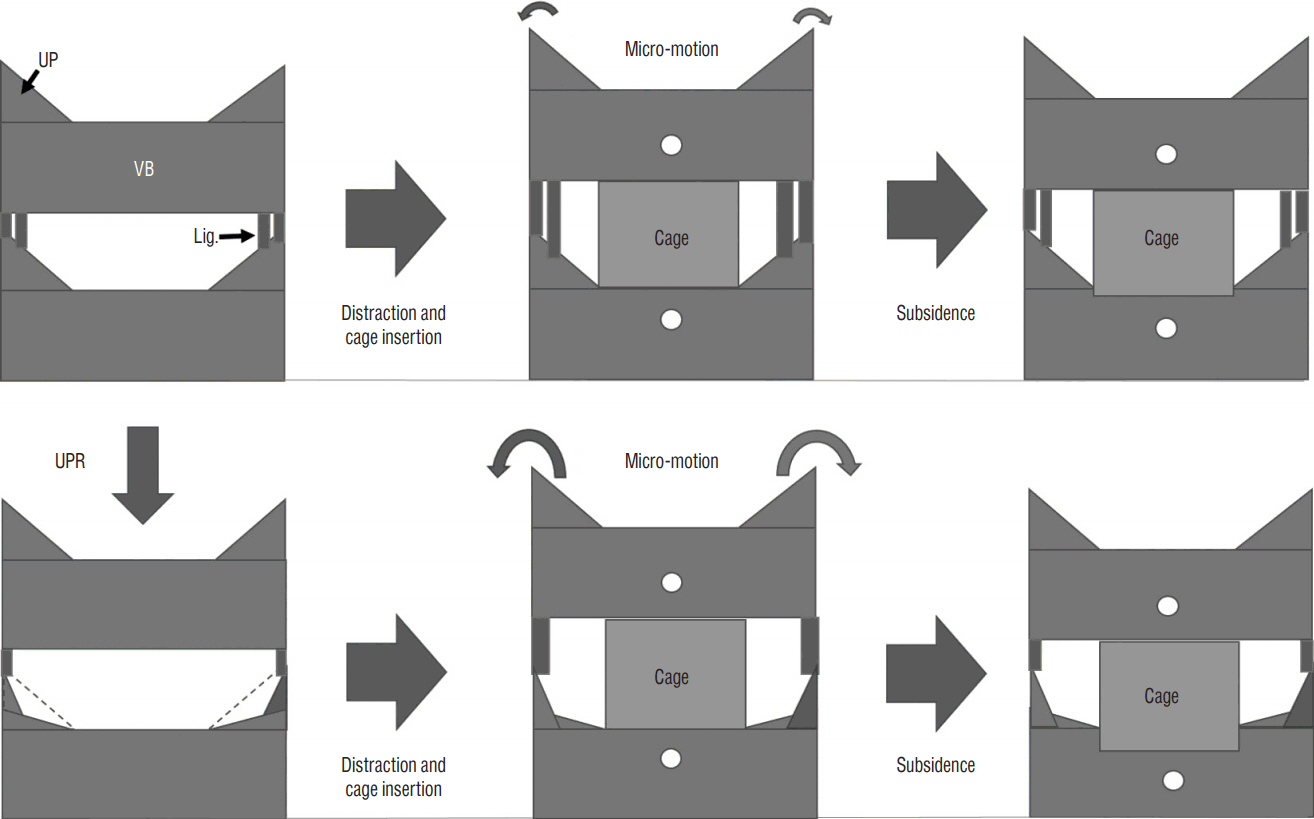
Fig. 1 Scheme illustrating the proposed relationship between uncinated process resection (UPR) and subsidence during anterior cervical discectomy and fusion (ACDF). The upper line demonstrates ACDF without UPR. Because of the intact uncovertebral joint, the segment achieves rigid stability. The lower line demonstrates ACDF with UPR. Through the disruption of bony structures and ligaments, UPR causes more micro-motion, which leads to the increase of subsidence. UP: uncinated process, VB: vertebral body, Lig.: ligaments surrounding uncovertebral joints.
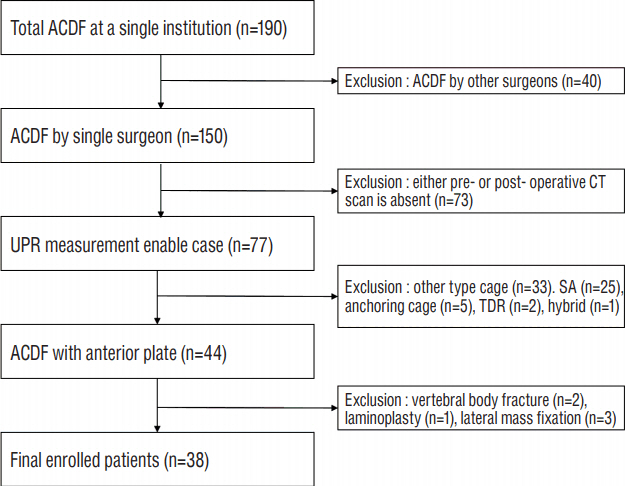
Fig. 2 Flow diagram depicting the patient inclusion process. ACDF: anterior cervical discectomy and fusion, CT: computed tomography, UPR: uncinated process resection area, SA: stand-alone cage, TDR: total disc replacement.
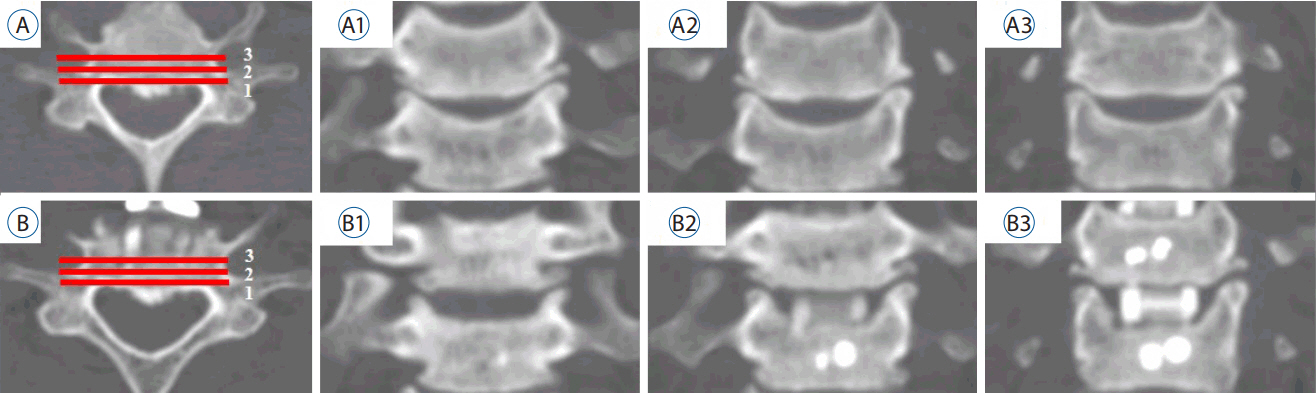
Fig. 3 Three sequential sections were obtained from the most posterior vertebral body toward the anterior direction. A: Pre-operative axial image at C6–7. B: postoperative axial image at the same level. A1–3: Pre-operative coronal images. B1–3: postoperative coronal images, with the number corresponding to the axial image (A and B).
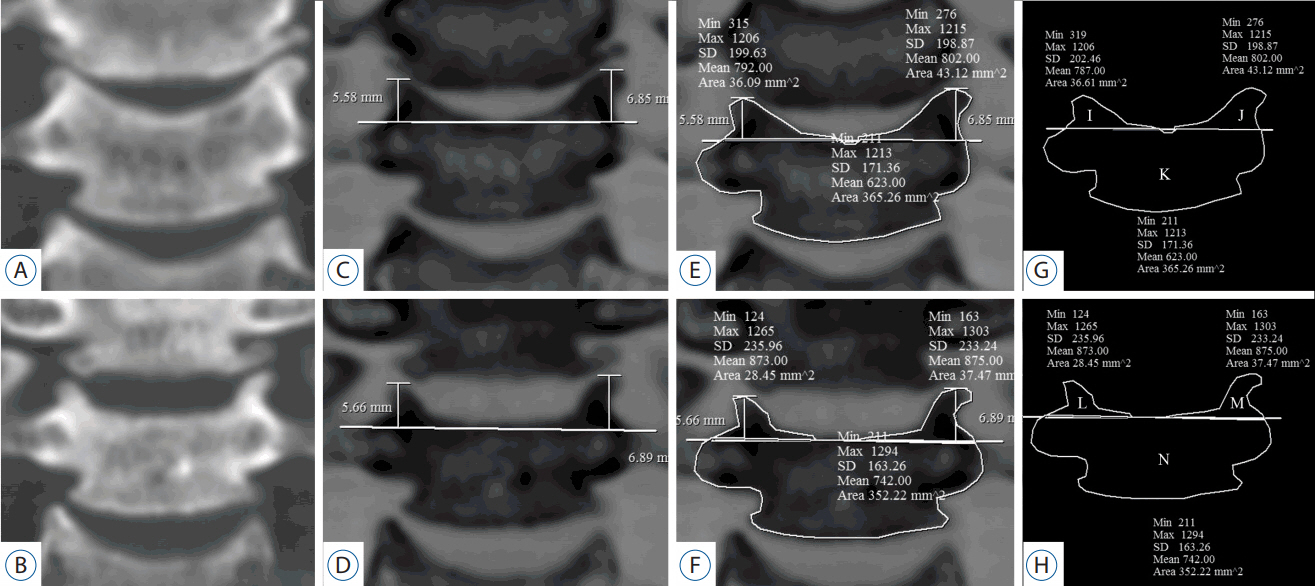
Fig. 4 Area measurements (uncinate process and vertebral body). A: Pre-operative (op), B: post-op coronal reformatted CT image at C5/6. C and D: The images are inverted. The base of the post-op UP was defined as a line connecting two points at the pre-op UP height. E and F: Measurements of bilateral UPs and VB. G and H: Schema of the UP and VB. I=pre-op right (Rt.) UP, J=pre-op left (Lt.) UP, K=pre-op VB, L=post-op Rt. UP, M=post-op Rt. UP, N=post-op VB. Rt. pUPR=1−L/I, the difference in VB=K−N. CT: computed tomography, UP: uncinate process, VB: vertebral body, pUPR: proportion of UPR to pre-UP.
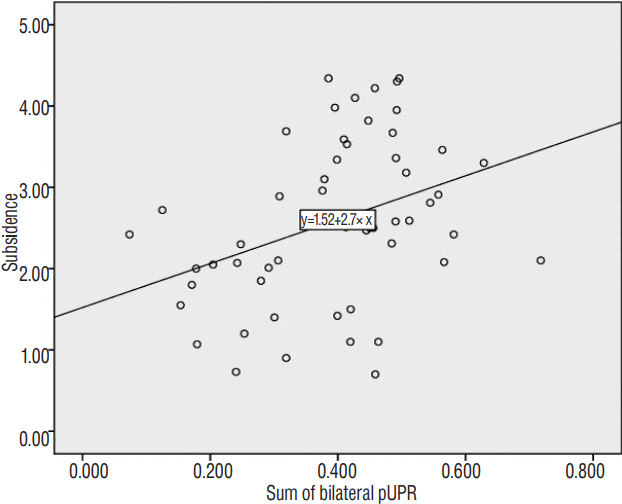
Fig. 5 Simple scatter graph and regression analysis between subsidence and the sum of bilateral pUPR (p=0.007; R2=0.133; adjusted R2=0.116). pUPR: proportion of uncinate process resection to pre-uncinate process area.
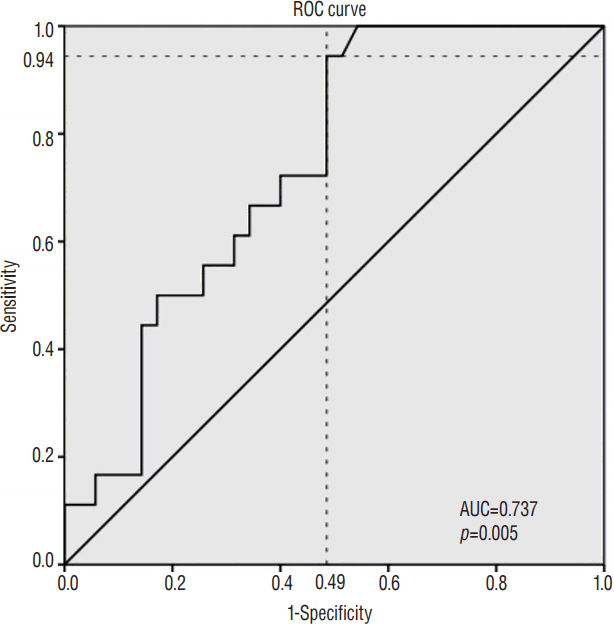
Fig. 6 Receiver operating characteristic (ROC) analysis was performed to determine the cut-off value of sum pUPR that induced significant subsidence. Sum pUPR above 0.38 could serve as a threshold for significantly increased risk of subsidence (p=0.005, AUC=0.737, sensitivity=94%, specificity=51%). pUPR: proportion of uncinate process resection (UPR) to pre-uncinate process (UP) area.
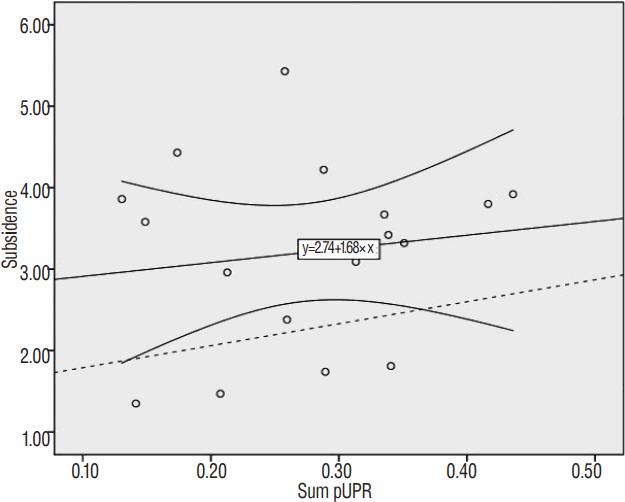
Fig. 7 Simple scatter plot: linear regression line with 95% confidence interval between subsidence and the sum of bilateral pUPR in ACDF with stand-alone PEEK cage (R=0.139, p=0.595). The dashed line represents the expected subsidence calculated by formula 2: subsidence=1.522+2.7×sum pUPR. pUPR: proportion of uncinate process resection to pre-uncinate process area, ACDF: anterior cervical discectomy and fusion, PEEK: polyether-ether-ketone.
Cited by 1 articles
-
Comparison between Anterior Cervical Decompression with Fusion and Posterior Cervical Fusion with Wide Facetectomy for Treatment of Severe Bony Foraminal Stenosis
Subum Lee, Dae-Chul Cho, Haemin Chon, Sung Woo Roh, Il Choi, Jin Hoon Park
J Korean Neurosurg Soc. 2021;64(4):552-561. doi: 10.3340/jkns.2020.0263.
Reference
-
References
1. Barsa P, Suchomel P. Factors affecting sagittal malalignment due to cage subsidence in standalone cage assisted anterior cervical fusion. Eur Spine J. 16:1395–1400. 2007.
Article2. Bartels RH, Donk RD, Feuth T. Subsidence of stand-alone cervical carbon fiber cages. Neurosurgery. 58:502–508. discussion 502–508. 2006.
Article3. Cannada LK, Scherping SC, Yoo JU, Jones PK, Emery SE. Pseudoarthrosis of the cervical spine: a comparison of radiographic diagnostic measures. Spine (Phila Pa 1976). 28:46–51. 2003.4. Chen TY, Crawford NR, Sonntag VK, Dickman CA. Biomechanical effects of progressive anterior cervical decompression. Spine (Phila Pa 1976). 26:6–13. discussion 14. 2001.
Article5. Ebraheim NA, Lu J, Haman SP, Yeasting RA. Anatomic basis of the anterior surgery on the cervical spine: relationships between uncus-artery-root complex and vertebral artery injury. Surg Radiol Anat. 20:389–392. 1998.
Article6. Francke EI, Demetropoulos CK, Agabegi SS, Truumees E, Herkowitz HN. Distractive force relative to initial graft compression in an in vivo anterior cervical discectomy and fusion model. Spine (Phila Pa 1976). 35:526–530. 2010.
Article7. Gercek E, Arlet V, Delisle J, Marchesi D. Subsidence of stand-alone cervical cages in anterior interbody fusion: warning. Eur Spine J. 12:513–516. 2003.
Article8. Joo YH, Lee JW, Kwon KY, Rhee JJ, Lee HK. Comparison of fusion with cage alone and plate instrumentation in two-level cervical degenerative disease. J Korean Neurosurg Soc. 48:342–346. 2010.
Article9. Kettler A, Wilke HJ, Claes L. Effects of neck movements on stability and subsidence in cervical interbody fusion: an in vitro study. J Neurosurg. 94(1 Suppl):97–107. 2001.
Article10. Kim WB, Hyun SJ, Choi H, Kim KJ, Jahng TA, Kim HJ. Long-term follow-up results of anterior cervical inter-body fusion with stand-alone cages. J Korean Neurosurg Soc. 59:385–391. 2016.
Article11. Kotani Y, McNulty PS, Abumi K, Cunningham BW, Kaneda K, McAfee PC. The role of anteromedial foraminotomy and the uncovertebral joints in the stability of the cervical spine. A biomechanical study. Spine (Phila Pa 1976). 23:1559–1565. 1998.
Article12. Lee YS, Kim YB, Park SW. Risk factors for postoperative subsidence of single-level anterior cervical discectomy and fusion: The significance of the preoperative cervical alignment. Spine (Phila Pa 1976). 39:1280–1287. 2014.
Article13. Lim TH, Kwon H, Jeon CH, Kim JG, Sokolowski M, Natarajan R, et al. Effect of endplate conditions and bone mineral density on the compressive strength of the graft-endplate interface in anterior cervical spine fusion. Spine (Phila Pa 1976). 26:951–956. 2001.
Article14. Liu Y, Luo X, Zhou J, Li N, Peng S, Rong P, et al. Prognosis of posterior osteophyte after anterior cervical decompression and fusion in patients with cervical spondylotic myelopathy using three-dimensional computed tomography study. Eur Spine J. 25:1861–1868. 2016.
Article15. Milne N. The role of zygapophysial joint orientation and uncinate processes in controlling motion in the cervical spine. J Anat. 178:189–201. 1991.16. Odom GL, Finney W, Woodhall B. Cervical disk lesions. J Am Med Assoc. 166:23–28. 1958.
Article17. Olivares-Navarrete R, Gittens RA, Schneider JM, Hyzy SL, Haithcock DA, Ullrich PF, et al. Osteoblasts exhibit a more differentiated phenotype and increased bone morphogenetic protein production on titanium alloy substrates than on poly-ether-ether-ketone. Spine J. 12:265–272. 2012.
Article18. Park JY, Choi KY, Moon BJ, Hur H, Jang JW, Lee JK. Subsidence after single-level anterior cervical fusion with a stand-alone cage. J Clin Neurosci. 33:83–88. 2016.
Article19. Pinder EM, Sharp DJ. Cage subsidence after anterior cervical discectomy and fusion using a cage alone or combined with anterior plate fixation. J Orthop Surg (Hong Kong). 24:97–100. 2016.
Article20. Schmieder K, Wolzik-Grossmann M, Pechlivanis I, Engelhardt M, Scholz M, Harders A. Subsidence of the wing titanium cage after anterior cervical interbody fusion: 2-year follow-up study. J Neurosurg Spine. 4:447–453. 2006.
Article21. Shen FH, Samartzis D, Khanna N, Goldberg EJ, An HS. Comparison of clinical and radiographic outcome in instrumented anterior cervical discectomy and fusion with or without direct uncovertebral joint decompression. Spine J. 4:629–635. 2004.
Article22. Smith GW, Robinson RA. The treatment of certain cervical-spine disorders by anterior removal of the intervertebral disc and interbody fusion. J Bone Joint Surg Am. 40-A:607–624. 1958.
Article23. Song KJ, Taghavi CE, Lee KB, Song JH, Eun JP. The efficacy of plate construct augmentation versus cage alone in anterior cervical fusion. Spine (Phila Pa 1976). 34:2886–2892. 2009.
Article24. Tanaka N, Fujimoto Y, An HS, Ikuta Y, Yasuda M. The anatomic relation among the nerve roots, intervertebral foramina, and intervertebral discs of the cervical spine. Spine (Phila Pa 1976). 25:286–291. 2000.
Article25. White AA, Panjabi MM. Clinical biomechanics of the spine. ed 2. Philadelphia: Lippincott;1990.26. Wu SH, Li Y, Zhang YQ, Li XK, Yuan CF, Hao YL, et al. Porous titanium-6 aluminum-4 vanadium cage has better osseointegration and less micromotion than a poly-ether-ether-ketone cage in sheep vertebral fusion. Artif Organs. 37:E191–E201. 2013.
Article27. Yang JJ, Yu CH, Chang BS, Yeom JS, Lee JH, Lee CK. Subsidence and nonunion after anterior cervical interbody fusion using a stand-alone polyetheretherketone (peek) cage. Clin Orthop Surg. 3:16–23. 2011.
Article28. Yao R, McLachlin SD, Rasoulinejad P, Gurr KR, Siddiqi F, Dunning CE, et al. Influence of graft size on spinal instability with anterior cervical plate fixation following in vitro flexion-distraction injuries. Spine J. 16:523–529. 2016.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Preoperative Radiographic Simulation for Partial Uncinate Process Resection during Anterior Cervical Discectomy and Fusion to Achieve Adequate Foraminal Decompression and Prevention of Vertebral Artery Injury
- Anterior Cervical Discectomy and Fusion Using a Stand-Alone Polyetheretherketone Cage Packed with Local Autobone : Assessment of Bone Fusion and Subsidence
- Subsidence of Polyetheretherketone Cage after Anterior Cervical Fusion
- How Subsidence Affects Clinical and Radiological Outcomes after Stand-Alone Anterior Cervical Discectomy and Fusion on Patients with Degenerative Cervical Disease? A Long-Term Follow-Up Study
- Effect of Osteoporosis on Clinical and Radiological Outcomes Following One-Level Anterior Cervical Discectomy and Fusion
