Prostate Artery Embolization: Treatment of Symptomatic Benign Prostatic Hyperplasia
- Affiliations
-
- 1Department of Radiology, Konkuk University School of Medicine, Seoul, Korea. psw0224@kuh.ac.kr
- KMID: 2457445
- DOI: http://doi.org/10.3348/jksr.2019.80.4.656
Abstract
- Prostatic artery embolization (PAE) is an emerging treatment option for lower urinary tract symptoms (LUTS) caused by benign prostatic hyperplasia (BPH). PAE is a minimally invasive technique and provides good results in BPH patients with moderate-to-severe LUTS. Most patients with BPH are old and have atherosclerosis. PAE can be technically challenging in these patients because of the tortuosity and small diameters of prostatic arteries. Therefore, patient selection is essential for successful results. To perform a safe procedure with no non-target embolization, precise knowledge of the prostatic arterial anatomy and meticulous techniques are important. A multidisciplinary approach by interventional radiologists and urologists is essential to achieve better outcomes.
MeSH Terms
Figure
-
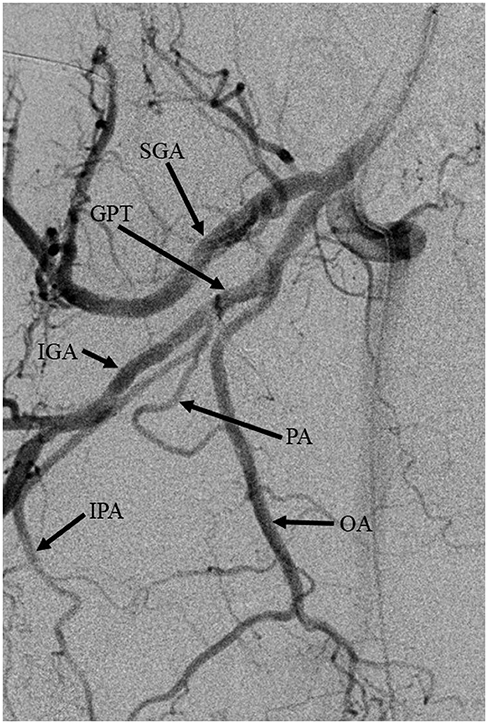
Fig. 1 An ipsilateral oblique view of the right internal iliac arteriogram demonstrates the anterior and posterior branches. GPT = gluteal-pudendal trunk, IGA = inferior gluteal artery, IPA = internal pudendal artery, OA = obturator artery, PA = prostatic artery, SGA = superior gluteal artery
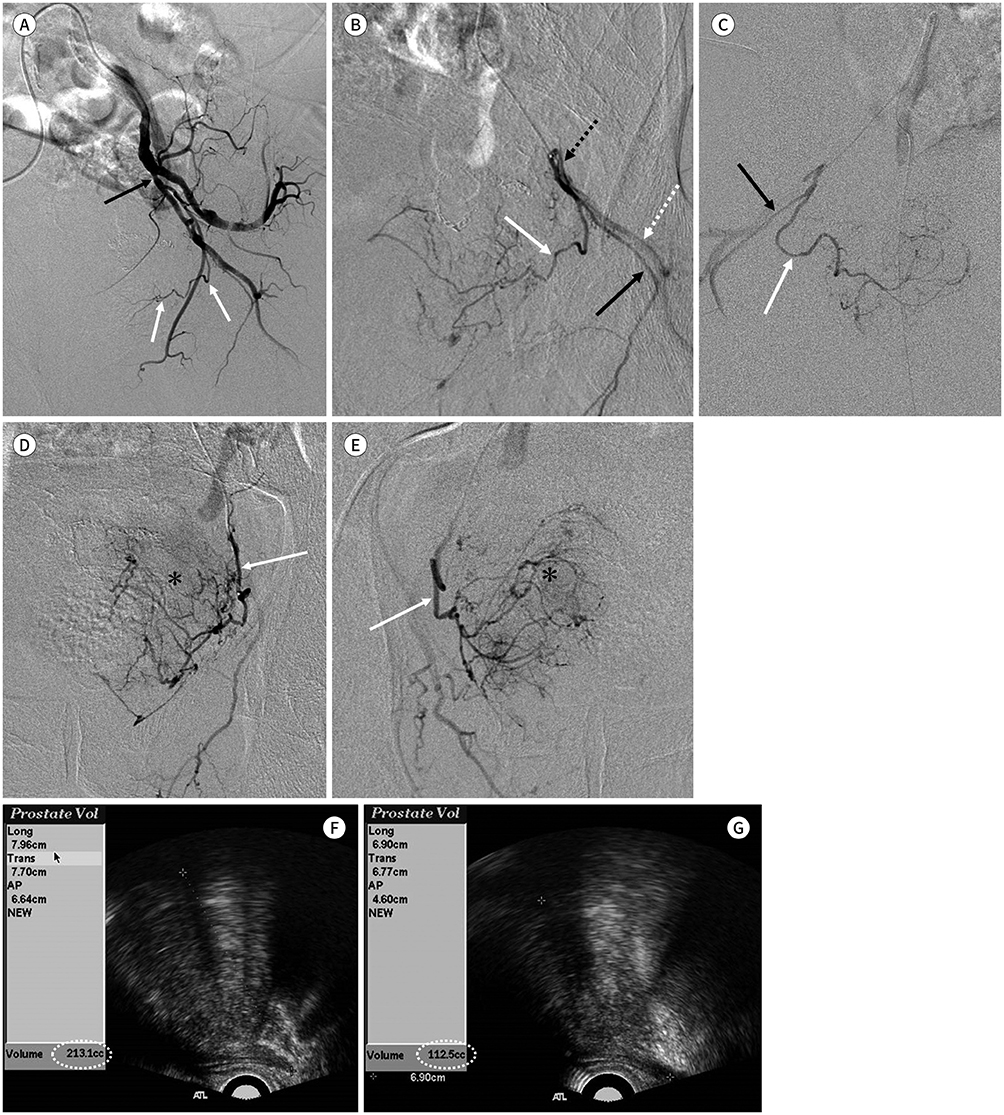
Fig. 2 A 76-year-old man with benign prostatic hyperplasia and lower urinary tract symptoms treated with PAE. A. An ipsilateral oblique view of the left internal iliac angiogram shows the prostatic artery (white arrows) originating from the anterior division of the internal iliac artery (black arrow). B. The left prostatic artery (white arrow) originating from the common trunk (black dotted arrow) of the internal pudendal artery (black arrow) and inferior gluteal artery (white dotted arrow). C. The right prostatic artery (white arrow) originating from the internal pudendal artery (black arrow). D, E. Selective angiography of both prostatic arteries (arrows) on anterior-posterior projection shows staining of the prostate gland (asterisks) with increased vascularity. A PAE with a microsphere (300–500 µm) was performed. PAE = prostatic artery embolization F, G. Trans-rectal ultrasound before (F) and after (G) PAE shows the prostatic volumes of 213.1 cc and 112.5 cc, respectively (a reduction of 47.2% after PAE).
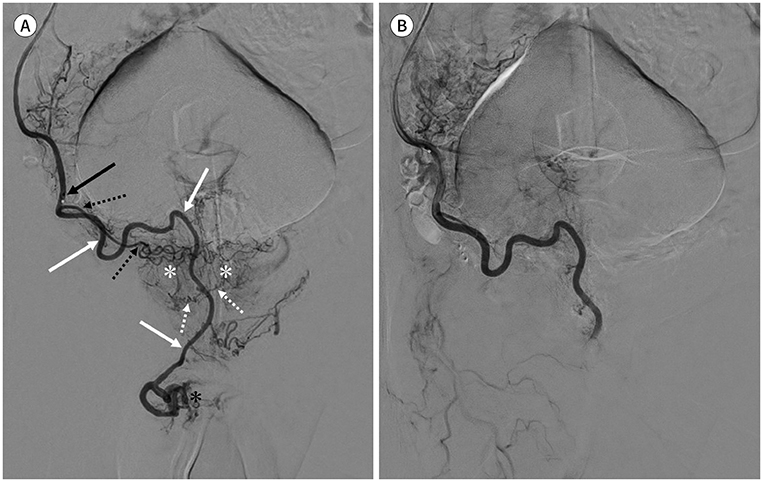
Fig. 3 A 58-year-old man with benign prostatic hyperplasia and lower urinary tract symptoms treated with prostatic artery embolization. A. Selective angiography of the right accessory pudendal artery (white arrows) on anterior-posterior projection shows parenchymal staining of both prostate lobes (white asterisks) supplied by fine prostatic branches (white dotted arrows). The tip of the microcatheter (black arrow) is positioned in the accessory pudendal artery just proximal to the origin of the inferior vesical artery (black dotted arrows). Arterial supply (black asterisk) to the penis is observed. B. After embolization, arterial supply to the penis and prostate gland was absent. Temporary erectile dysfunction had occurred, which improved 3 weeks later without any specific treatment.
Cited by 1 articles
-
Current trends in minimally invasive surgery for benign prostatic hyperplasia
Min Soo Choo, Hwancheol Son
J Korean Med Assoc. 2020;63(2):119-125. doi: 10.5124/jkma.2020.63.2.119.
Reference
-
1. McWilliams JP, Kuo MD, Rose SC, Bagla S, Caplin DM, Cohen EI, et al. Society of Interventional Radiology position statement: prostate artery embolization for treatment of benign disease of the prostate. J Vasc Interv Radiol. 2014; 25:1349–1351.2. McVary KT, Roehrborn CG, Avins AL, Barry MJ, Bruskewitz RC, Donnell RF, et al. Update on AUA guideline on the management of benign prostatic hyperplasia. J Urol. 2011; 185:1793–1803.3. Carnevale FC, Antunes AA. Prostatic artery embolization for enlarged prostates due to benign prostatic hyperplasia. How I do it. Cardiovasc Intervent Radiol. 2013; 36:1452–1463.4. Mebust WK, Holtgrewe HL, Cockett AT, Peters PC. Transurethral prostatectomy: immediate and postoperative complications. a cooperative study of 13 participating institutions evaluating 3,885 patients. 1989. J Urol. 2002; 167:999–1003. discussion 1004.5. Westenberg A, Gilling P, Kennett K, Frampton C, Fraundorfer M. Holmium laser resection of the prostate versus transurethral resection of the prostate: results of a randomized trial with 4-year minimum long-term followup. J Urol. 2004; 172:616–619.6. Rastinehad AR, Caplin DM, Ost MC, VanderBrink BA, Lobko I, Badlani GH, et al. Selective arterial prostatic embolization (SAPE) for refractory hematuria of prostatic origin. Urology. 2008; 71:181–184.7. DeMeritt JS, Elmasri FF, Esposito MP, Rosenberg GS. Relief of benign prostatic hyperplasia-related bladder outlet obstruction after transarterial polyvinyl alcohol prostate embolization. J Vasc Interv Radiol. 2000; 11:767–770.8. Sun F, Sánchez FM, Crisóstomo V, Lima JR, Luis L, García-Martínez V, et al. Benign prostatic hyperplasia: transcatheter arterial embolization as potential treatment--preliminary study in pigs. Radiology. 2008; 246:783–789.9. Jeon GS, Won JH, Lee BM, Kim JH, Ahn HS, Lee EJ, et al. The effect of transarterial prostate embolization in hormone-induced benign prostatic hyperplasia in dogs: a pilot study. J Vasc Interv Radiol. 2009; 20:384–390.10. Carnevale FC, Antunes AA, Da Motta Leal Filho JM, De Oliveira Cerri LM, Baroni RH, Marcelino AS, et al. Prostatic artery embolization as a primary treatment for benign prostatic hyperplasia: preliminary results in two patients. Cardiovasc Intervent Radiol. 2010; 33:355–361.11. Bagla S, Martin CP, Van Breda A, Sheridan MJ, Sterling KM, Papadouris D, et al. Early results from a United States trial of prostatic artery embolization in the treatment of benign prostatic hyperplasia. J Vasc Interv Radiol. 2014; 25:47–52.12. Carnevale FC, Da Motta-Leal-Filho JM, Antunes AA, Baroni RH, Marcelino AS, Cerri LM, et al. Quality of life and clinical symptom improvement support prostatic artery embolization for patients with acute urinary retention caused by benign prostatic hyperplasia. J Vasc Interv Radiol. 2013; 24:535–542.13. Gao YA, Huang Y, Zhang R, Yang YD, Zhang Q, Hou M, et al. Benign prostatic hyperplasia: prostatic arterial embolization versus transurethral resection of the prostate--a prospective, randomized, and controlled clinical trial. Radiology. 2014; 270:920–928.14. De Assis AM, Moreira AM, De Paula Rodrigues VC, Yoshinaga EM, Antunes AA, Harward SH, et al. Prostatic artery embolization for treatment of benign prostatic hyperplasia in patients with prostates > 90 g: a prospective single-center study. J Vasc Interv Radiol. 2015; 26:87–93.15. Kurbatov D, Russo GI, Lepetukhin A, Dubsky S, Sitkin I, Morgia G, et al. Prostatic artery embolization for prostate volume greater than 80 cm3: results from a single-center prospective study. Urology. 2014; 84:400–404.16. Bilhim T, Pisco JM, Rio Tinto H, Fernandes L, Pinheiro LC, Furtado A, et al. Prostatic arterial supply: anatomic and imaging findings relevant for selective arterial embolization. J Vasc Interv Radiol. 2012; 23:1403–1415.17. Sun F, Crisóstomo V, Báez-Díaz C, Sánchez FM. Prostatic artery embolization (PAE) for symptomatic benign prostatic hyperplasia (BPH): part 2, insights into the technical rationale. Cardiovasc Intervent Radiol. 2016; 39:161–169.18. Jones P, Rai BP, Nair R, Somani BK. Current status of prostate artery embolization for lower urinary tract symptoms: review of world literature. Urology. 2015; 86:676–681.19. Bilhim T, Tinto HR, Fernandes L, Martins Pisco J. Radiological anatomy of prostatic arteries. Tech Vasc Interv Radiol. 2012; 15:276–285.20. Martins Pisco J J, Pereira J, Rio Tinto H, Fernandes L, Bilhim T. How to perform prostatic arterial embolization. Tech Vasc Interv Radiol. 2012; 15:286–289.21. Fernandes L, Rio Tinto H, Pereira J, Duarte M, Bilhim T, Martins Pisco J. Prostatic arterial embolization: postprocedural follow-up. Tech Vasc Interv Radiol. 2012; 15:294–299.22. A Pereira J, Bilhim T, Duarte M, Rio Tinto H, Fernandes L, Martins Pisco J. Patient selection and counseling before prostatic arterial embolization. Tech Vasc Interv Radiol. 2012; 15:270–275.23. Pisco JM, Rio Tinto H, Campos Pinheiro L, Bilhim T, Duarte M, Fernandes L, et al. Embolisation of prostatic arteries as treatment of moderate to severe lower urinary symptoms (LUTS) secondary to benign hyperplasia: results of short- and mid-term follow-up. Eur Radiol. 2013; 23:2561–2572.24. Bhatia S, Harward SH, Sinha VK, Narayanan G. Prostate artery embolization via transradial or transulnar versus transfemoral arterial access: technical results. J Vasc Interv Radiol. 2017; 28:898–905.25. Bagla S, Rholl KS, Sterling KM, Van Breda A, Papadouris D, Cooper JM, et al. Utility of cone-beam CT imaging in prostatic artery embolization. J Vasc Interv Radiol. 2013; 24:1603–1607.26. Pisco J, Campos Pinheiro L, Bilhim T, Duarte M, Rio Tinto H, Fernandes L, et al. Prostatic arterial embolization for benign prostatic hyperplasia: short- and intermediate-term results. Radiology. 2013; 266:668–677.27. Bilhim T, Pisco J, Campos Pinheiro L, Rio Tinto H, Fernandes L, Pereira JA, et al. Does polyvinyl alcohol particle size change the outcome of prostatic arterial embolization for benign prostatic hyperplasia? Results from a single-center randomized prospective study. J Vasc Interv Radiol. 2013; 24:1595–1602.e1.28. Laurent A. Microspheres and nonspherical particles for embolization. Tech Vasc Interv Radiol. 2007; 10:248–256.29. Hwang JH, Park SW, Chang IS, Jung SI, Jeon HJ, Lho YS, et al. Comparison of nonspherical polyvinyl alcohol particles and microspheres for prostatic arterial embolization in patients with benign prostatic hyperplasia. Biomed Res Int. 2017; 2017:8732351.30. Bhatia S, Sinha V, Bordegaray M, Kably I, Harward S, Narayanan G. Role of coil embolization during prostatic artery embolization: incidence, indications, and safety profile☆. J Vasc Interv Radiol. 2017; 28:656–664.e3.31. Pisco JM, Pinheiro LC, Bilhim T, Duarte M, Mendes JR, Oliveira AG. Prostatic arterial embolization to treat benign prostatic hyperplasia. J Vasc Interv Radiol. 2011; 22:11–19. quiz 20.32. Bilhim T, Pisco J, Rio Tinto H, Fernandes L, Campos Pinheiro L, Duarte M, et al. Unilateral versus bilateral prostatic arterial embolization for lower urinary tract symptoms in patients with prostate enlargement. Cardiovasc Intervent Radiol. 2013; 36:403–411.33. Henry BM, Pekala PA, Vikse J, Sanna B, Skinningsrud B, Saganiak K, et al. Variations in the arterial blood supply to the penis and the accessory pudendal artery: a meta-analysis and review of implications in radical prostatectomy. J Urol. 2017; 198:345–353.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Possibility of the Expert System for Benign Prostatic Hyperplasia in Symptomatic Prostatism, Using Symptom Scores, Prostatic Size and Other Factors
- A Prominently Large Glans penis as a Possible sign of Benign Prostatic Hyperplasia
- The effect of prazosin as a first-line therapy for the symptomatic benign prostatichypertrophy
- The role of serum prostate specific antigen in prostatic cancer and benign prostatic hyperplasia
- The Experience with Combination of Finasteride and Tamsulosin on Benign Prostatic Hyperplasia
