Cost effectiveness analysis of HPV primary screening and dual stain cytology triage compared with cervical cytology
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Faculty of Medicine, Chulalongkorn University, Bangkok, Thailand. wichaiterm@yahoo.com
- 2Department of Obstetrics and Gynecology, Faculty of Medicine, Srinakharinwirot University, Nakhonnayok, Thailand.
- KMID: 2457130
- DOI: http://doi.org/10.3802/jgo.2019.30.e17
Abstract
OBJECTIVES
To assess the clinical and cost-effectiveness of human papillomavirus (HPV) primary screening triage with p16/Ki-67 dual stain cytology compared to cytology.
METHODS
We conducted an Excel®-based budget impact model to estimate the preinvasive and invasive cervical cancer cases identified, mortality rate, direct medical costs, quality-adjusted life years (QALYs) and the incremental cost-effectiveness analysis of two strategies from the healthcare payer perspective. The study population is a cohort of women 30-65 years of age presenting for cervical screening.
RESULTS
HPV primary screening triage with p16/Ki-67 dual stain showed higher sensitivity without losing specificity compared to conventional Pap smear. The improving the screening performance leads to decrease the prevalence of precancerous lesion, annual incidence and mortality of cervical cancer. The incidence of cervical cancer case detected by new algorithm compared with conventional method were 31,607 and 38,927, respectively. In addition, the new algorithm was more effective and more costly (average QALY 24.03, annual cost $13,262,693) than conventional cytology (average QALY 23.98, annual cost $7,713,251). The incremental cost-effective ratio (ICER) per QALY gained was $1,395. The sensitivity analysis showed if the cost of cytology and HPV test increased three times, the ICER would fall to $303/QALY gained and increased to $4,970/QALY gained, respectively.
CONCLUSIONS
Our model results suggest that screening by use of HPV genotyping test as a primary screening test combined with dual stain cytology as the triage of HPV positive women in Thai population 30-65 years old is expected to be more cost-effective than conventional Pap cytology.
Keyword
MeSH Terms
-
Asian Continental Ancestry Group
Biomarkers
Budgets
Cohort Studies
Cost-Benefit Analysis*
Delivery of Health Care
Early Detection of Cancer
Female
Human Papillomavirus DNA Tests
Humans
Incidence
Mass Screening*
Methods
Mortality
Papanicolaou Test
Prevalence
Quality-Adjusted Life Years
Sensitivity and Specificity
Triage*
Uterine Cervical Neoplasms
Biomarkers
Figure
-
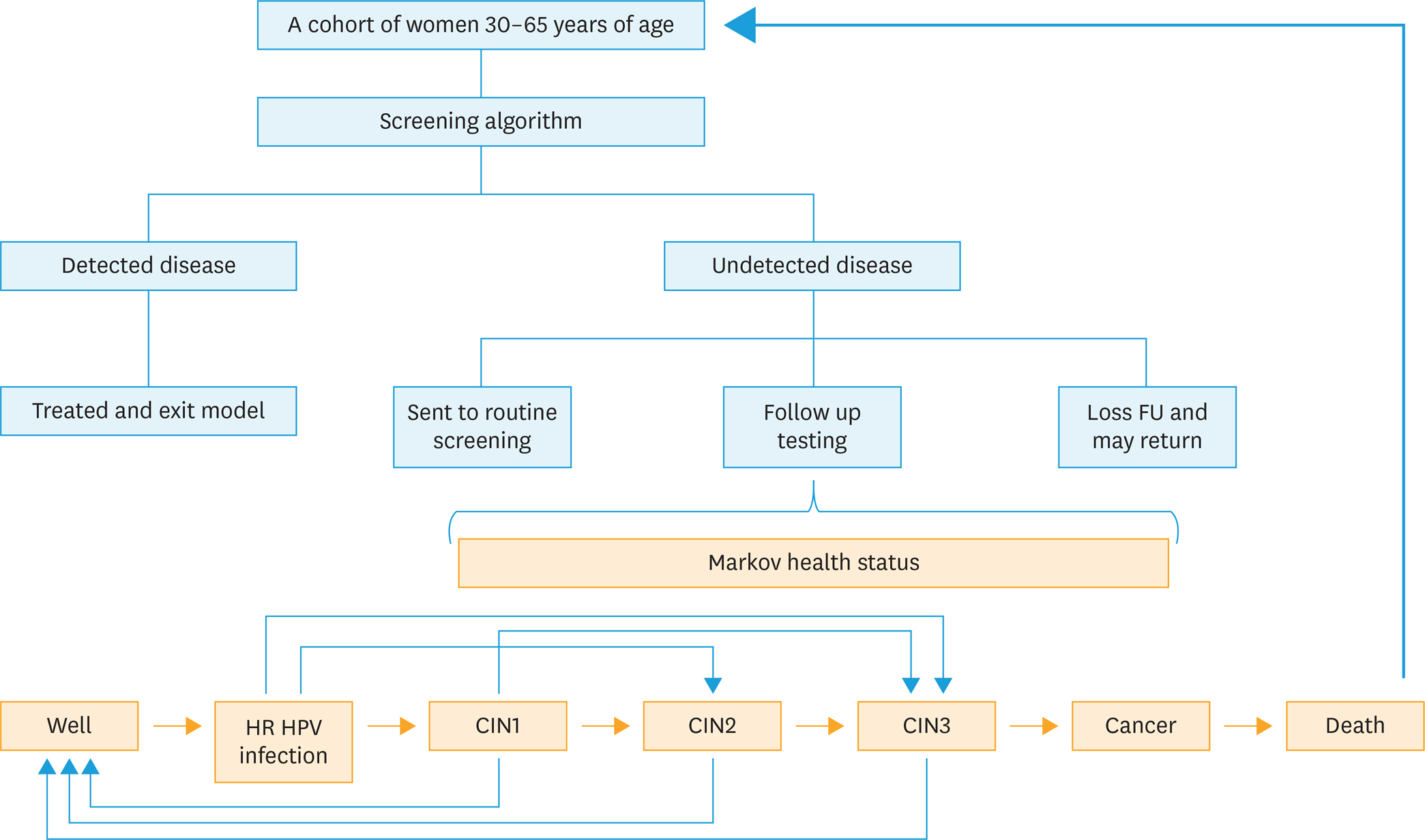
Fig. 1. A model of the patient flow through a cervical cancer screening. CIN, cervical intraepithelial neoplasia; FU, follow up; HPV, human papillomavirus.
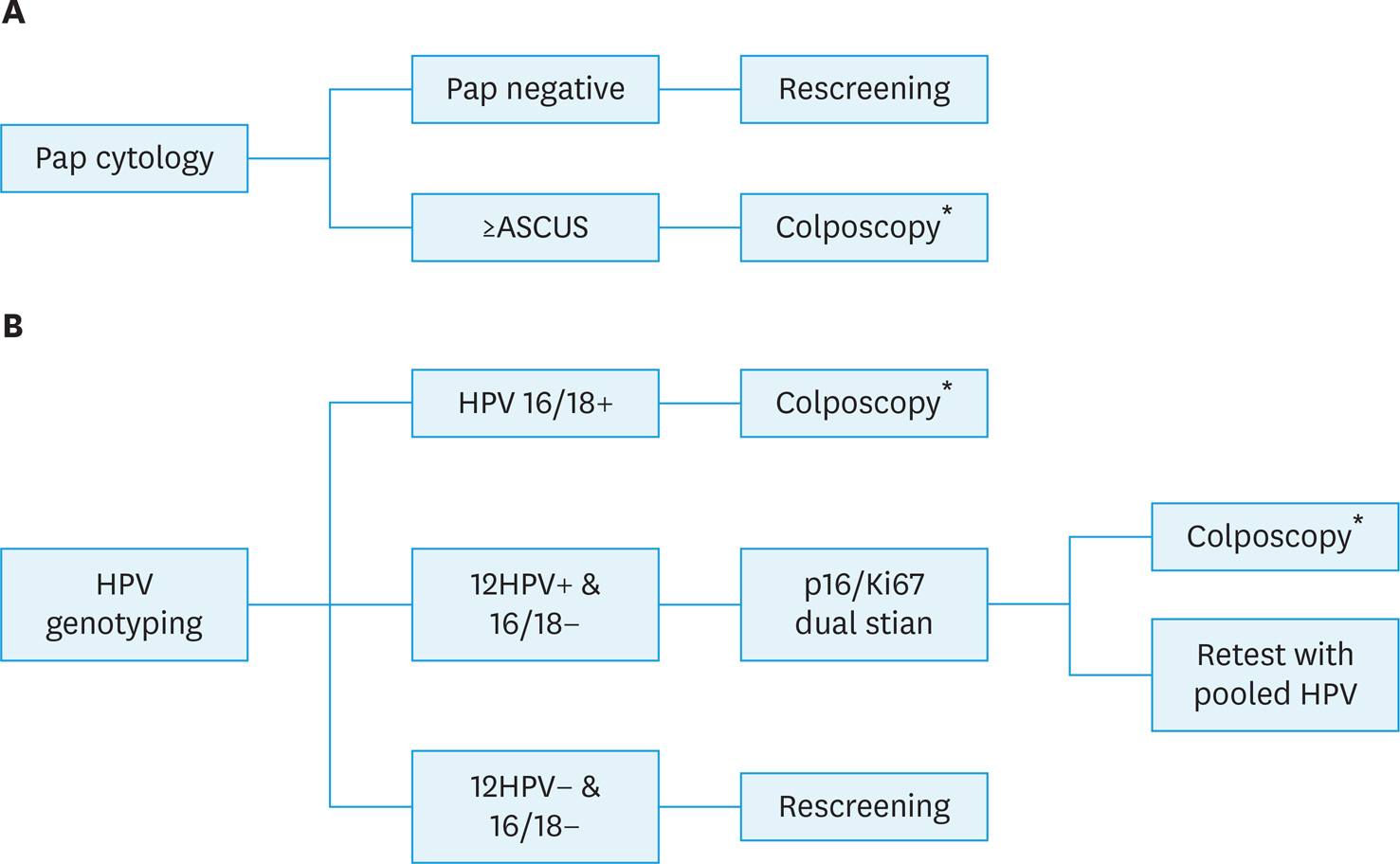
Fig. 2. Screening model. (A) Cytology: screening with conventional cytology. (B) HPV/dual stain: HPV DNA test with genotyping 16&18 plus triage with p16/Ki-67 dual stain. ASCUS, atypical squamous cells of undetermined significance; CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus; ICC, invasive cervical cancer. * Women with negative colposcopy return to routine screening, women with CIN or ICC were referred to treatment.
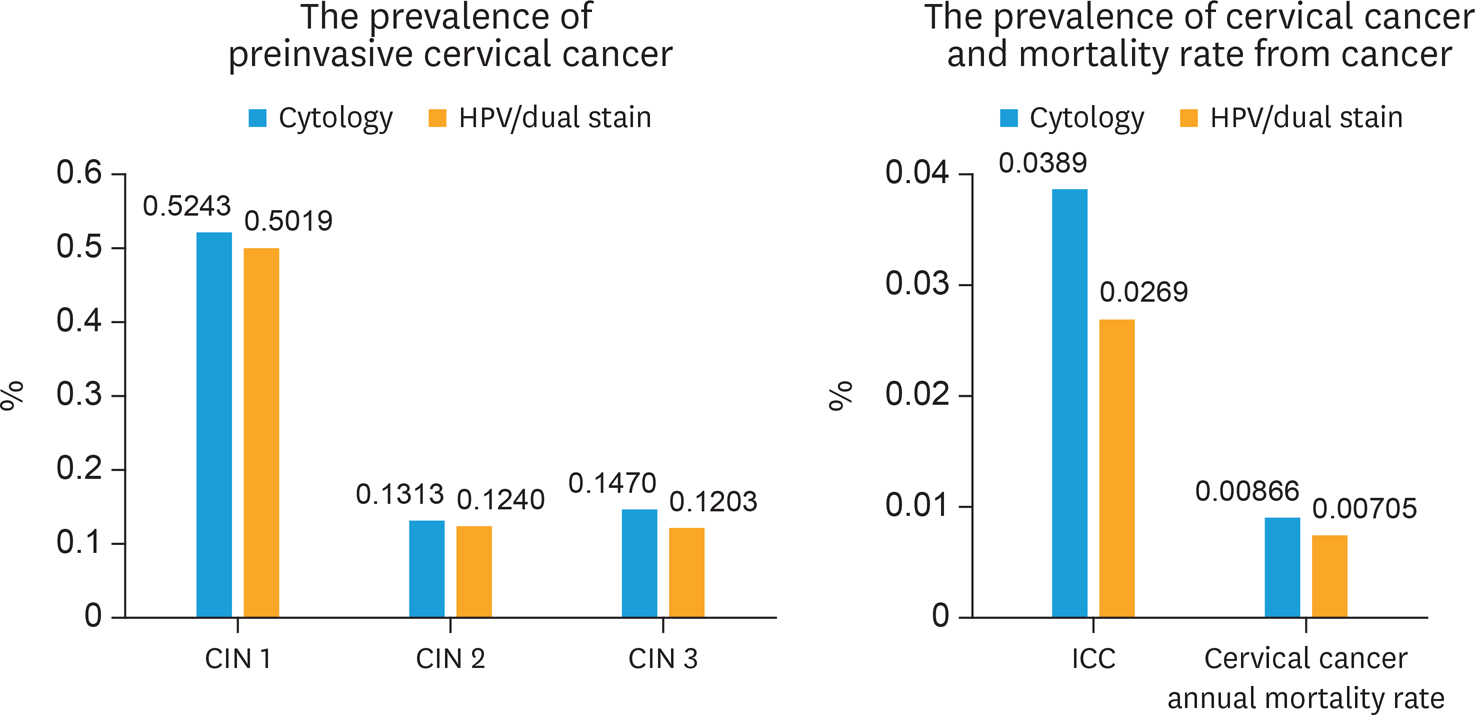
Fig. 3. The prevalence of preinvasive cervical cancer, cervical cancer, and mortality rate from cancer. CIN, cervical intraepithelial neoplasia; HPV, human papillomavirus.
Reference
-
References
1. Bruni L, Barrionuevo-Rosas L, Albero G, Serrano B, Mena M, Gómez D, et al. Human papillomavirus and related diseases in the world. Summary report [Internet]. Barcelona: ICO/IARC Information Centre on HPV and Cancer (HPV Information Centre);2017. July 27 [cited 2018 Jan 20]. Available from:. http://www.hpvcentre.net/statistics/reports/XWX.pdf.2. Termrungruanglert W, Khemapech N, Tantitamit T, Sangrajrang S, Havanond P, Laowahutanont P. Cost-effectiveness analysis study of HPV testing as a primary cervical cancer screening in Thailand. Gynecol Oncol Rep. 2017; 22:58–63.
Article3. Ikenberg H, Bergeron C, Schmidt D, Griesser H, Alameda F, Angeloni C, et al. Screening for cervical cancer precursors with p16/Ki-67 dual-stained cytology: results of the PALMS study. J Natl Cancer Inst. 2013; 105:1550–7.
Article4. Wright TC Jr, Behrens CM, Ranger-Moore J, Rehm S, Sharma A, Stoler MH, et al. Triaging HPV-positive women with p16/Ki-67 dual-stained cytology: results from a sub-study nested into the ATHENA trial. Gynecol Oncol. 2017; 144:51–6.
Article5. Uijterwaal MH, Polman NJ, Witte BI, van Kemenade FJ, Rijkaart D, Berkhof J, et al. Triaging HPV-positive women with normal cytology by p16/Ki-67 dual-stained cytology testing: baseline and longitudinal data. Int J Cancer. 2015; 136:2361–8.
Article6. Wentzensen N, Fetterman B, Castle PE, Schiffman M, Wood SN, Stiemerling E, et al. p16/Ki-67 dual stain cytology for detection of cervical precancer in HPV-positive women. J Natl Cancer Inst. 2015; 107:djv257.
Article7. Ovestad IT, Dalen I, Hansen E, Loge JL, Dybdahl BM, Dirdal MB, et al. Clinical value of fully automated p16/Ki-67 dual staining in the triage of HPV-positive women in the Norwegian Cervical Cancer Screening Program. Cancer Cytopathol. 2017; 125:283–91.
Article8. World Bank Group. Population, total 2015 [Internet]. Washington, D.C.: World Bank Group;c2018. [cited 2018 Jan 8]. Available from:. http://data.worldbank.org/indicator/SP.POP.TOTL?view=chart.9. Ministry of Public Health. Cervical cancer screening rate in women aged 30–60 years [Internet]. Muang Nonthaburi: Ministry of Public Health;c2018. [cited 2018 Jan 20]. Available from:. https://hdcservice.moph.go.th/hdc/reports/report.php?source=pformated/format1.php&cat_id=6966b0664b89805a484d7ac96c6edc48&id=4eab25b045dc0a9453d85c98dc2fdef0.10. National Statistical Office; United Nations Children's Fund; Ministry of Public Health; National Health Security Office; Thai Health Promotion Foundation; International Health Policy Program. Thailand monitoring the situation of children and women: multiple indicator cluster survey 2012 [Internet]. Laksi Bangkok: National Statistical Office;c2013. [cited 2018 Jan 20]. Available from:. http://web.nso.go.th/en/survey/monitoring/data/monitoring_full_report_2012.pdf.11. Schneider A, Hoyer H, Lotz B, Leistritza S, Kühne-Heid R, Nindl I, et al. Screening for high-grade cervical intraepithelial neoplasia and cancer by testing for high-risk HPV, routine cytology or colposcopy. Int J Cancer. 2000; 89:529–34.
Article12. Tantitamit T, Termrungruanglert W, Khemapech N, Havanond P. A model approach for assessing the benefits of HPV testing against cytology in screening for cervical cancer precursors in Thailand. Asian Pac J Cancer Prev. 2017; 18:1271–5.13. Friedlander M, Grogan M. U.S. Preventative Services Task Force. Guidelines for the treatment of recurrent and metastatic cervical cancer. Oncologist. 2002; 7:342–7.
Article14. Mandelblatt JS, Lawrence WF, Womack SM, Jacobson D, Yi B, Hwang YT, et al. Benefits and costs of using HPV testing to screen for cervical cancer. JAMA. 2002; 287:2372–81.
Article15. United Nations, Department of Economic and Social Affairs, Population Division (UNPD). World population prospects: the 2015 revision, key findings and advance tables. New York, NY: United Nations;2015.16. Wright TC Jr, Stoler MH, Sharma A, Zhang G, Behrens C, Wright TL, et al. Evaluation of HPV-16 and HPV-18 genotyping for the triage of women with high-risk HPV+ cytology-negative results. Am J Clin Pathol. 2011; 136:578–86.
Article17. Kulasingam SL, Benard S, Barnabas RV, Largeron N, Myers ER. Adding a quadrivalent human papillomavirus vaccine to the UK cervical cancer screening programme: a cost-effectiveness analysis. Cost Eff Resour Alloc. 2008; 6:4.
Article18. Myers ER, Green S, Lipkus I. Patient preferences for health states related to HPV infection: visual analog scales vs time trade-off elicitation. Proceedings of 21st International Papillomavirus Conference. 2004 Feb 20–27; Mexico City. International Papillomavirus Society;. 2004. Abstract 542.19. Termrungruanglert W, Khemapech N, Havanond P, Pillsbury M, Shcheprov A, Numuang K, et al. Impact of vaccination: Health impact and cost-effectiveness to make informed policy decision on the introduction of human papillomavirus (HPV) vaccine to the national immunization Program (Nip) in Thailand. Value Health. 2014; 17:A737.
Article20. National Institute for Health and Care Excellence. NICE process and methods guides. Guide to the methods of technology appraisal 2013. London: National Institute for Health and Care Excellence;2013.21. Ogilvie GS, van Niekerk D, Krajden M, Smith LW, Cook D, Gondara L, et al. Effect of screening with primary cervical HPV testing vs cytology testing on high-grade cervical intraepithelial neoplasia at 48 months: the HPV FOCAL randomized clinical trial. JAMA. 2018; 320:43–52.
Article22. Tjalma WA, Kim E, Vandeweyer K. The impact on women's health and the cervical cancer screening budget of primary HPV screening with dual-stain cytology triage in Belgium. Eur J Obstet Gynecol Reprod Biol. 2017; 212:171–81.
Article23. World Health Organization. Macroeconomic and health: investing in health for economic development: report for the commission on macroeconomics and health. Geneva: World Health Organization;2001.24. Wright TC Jr, Stoler MH, Behrens CM, Apple R, Derion T, Wright TL. The ATHENA human papillomavirus study: design, methods, and baseline results. Am J Obstet Gynecol. 2012; 206:46. e1–11.
Article25. Cox JT, Castle PE, Behrens CM, Sharma A, Wright TC Jr, Cuzick J. Athena HPV Study Group. Comparison of cervical cancer screening strategies incorporating different combinations of cytology, HPV testing, and genotyping for HPV 16/18: results from the ATHENA HPV study. Am J Obstet Gynecol. 2013; 208:184. e1–11.
Article26. Luyten A, Scherbring S, Reinecke-Lüthge A, Braun BE, Pietralla M, Theiler K, et al. Risk-adapted primary HPV cervical cancer screening project in Wolfsburg, Germany–experience over 3 years. J Clin Virol. 2009; 46(Suppl 3):S5–10.27. Petry KU, Menton S, Menton M, van Loenen-Frosch F, de Carvalho Gomes H, Holz B, et al. Inclusion of HPV testing in routine cervical cancer screening for women above 29 years in Germany: results for 8466 patients. Br J Cancer. 2003; 88:1570–7.
Article28. Klug SJ, Hukelmann M, Hollwitz B, Düzenli N, Schopp B, Petry KU, et al. Prevalence of human papillomavirus types in women screened by cytology in Germany. J Med Virol. 2007; 79:616–25.
Article29. Cuzick J, Myers O, Hunt WC, Saslow D, Castle PE, Kinney W, et al. Human papillomavirus testing 2007–2012: co-testing and triage utilization and impact on subsequent clinical management. Int J Cancer. 2015; 136:2854–63.30. Smith JS, Lindsay L, Hoots B, Keys J, Franceschi S, Winer R, et al. Human papillomavirus type distribution in invasive cervical cancer and high-grade cervical lesions: a meta-analysis update. Int J Cancer. 2007; 121:621–32.
Article31. World Bank Group. Death rate, crude (per 1,000 people) 2014 [Internet]. Washington, D.C.: World Bank Group;c2018. [cited 2018 Jan 20]. Available from:. http://data.worldbank.org/indicator/SP.DYN.CDRT.IN.32. Chen T, Jansen L, Gondos A, Emrich K, Holleczek B, Luttmann S, et al. Survival of cervical cancer patients in Germany in the early 21st century: a period analysis by age, histology, and stage. Acta Oncol. 2012; 51:915–21.
Article33. Holowaty P, Miller AB, Rohan T, To T. Natural history of dysplasia of the uterine cervix. J Natl Cancer Inst. 1999; 91:252–8.
Article34. Insinga RP, Dasbach EJ, Elbasha EH. Epidemiologic natural history and clinical management of human papillomavirus (HPV) disease: a critical and systematic review of the literature in the development of an HPV dynamic transmission model. BMC Infect Dis. 2009; 9:119.
Article35. Insinga RP, Dasbach EJ, Elbasha EH, Liaw KL, Barr E. Progression and regression of incident cervical HPV 6, 11, 16 and 18 infections in young women. Infect Agent Cancer. 2007; 2:15.
Article36. Insinga RP, Perez G, Wheeler CM, Koutsky LA, Garland SM, Leodolter S, et al. Incident cervical HPV infections in young women: transition probabilities for CIN and infection clearance. Cancer Epidemiol Biomarkers Prev. 2011; 20:287–96.
Article37. Kataja V, Syrjänen K, Mäntyjärvi R, Väyrynen M, Syrjänen S, Saarikoski S, et al. Prospective follow-up of cervical HPV infections: life table analysis of histopathological, cytological and colposcopic data. Eur J Epidemiol. 1989; 5:1–7.
Article38. Khan MJ, Castle PE, Lorincz AT, Wacholder S, Sherman M, Scott DR, et al. The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice. J Natl Cancer Inst. 2005; 97:1072–9.
Article39. Matsumoto K, Yasugi T, Oki A, Fujii T, Nagata C, Sekiya S, et al. IgG antibodies to HPV16, 52, 58 and 6 L1-capsids and spontaneous regression of cervical intraepithelial neoplasia. Cancer Lett. 2006; 231:309–13.
Article40. Bulkmans NW, Berkhof J, Bulk S, Bleeker MC, van Kemenade FJ, Rozendaal L, et al. High-risk HPV type-specific clearance rates in cervical screening. Br J Cancer. 2007; 96:1419–24.
Article41. Termrungruanglert W, Havanond P, Khemapech N, Lertmaharit S, Pongpanich S, Khorprasert C, et al. Cost and effectiveness evaluation of prophylactic HPV vaccine in developing countries. Value Health. 2012; 15:S29–34.
Article42. Lier D, Jacobs P. An economic analysis of the introduction of liquid-based cytology (LBC) and human papillomavirus (HPV) testing in Alberta [Internet]. Calgary: Alberta Cervical Cancer Screening Program;c2018. [cited 2018 Jan 20]. Available from:. https://www.albertahealthservices.ca/findhealth/service.43. Termrungruanglert W, Havanond P, Khemapech N, Lertmaharit S, Pongpanich S, Jirakorbchaipong P, et al. Model for predicting the burden and cost of treatment in cervical cancer and HPV-related diseases in Thailand. Eur J Gynaecol Oncol. 2012; 33:391–4.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Clinical Evaluation of Triple Combined Test [ Cytology, HPV DNA Test, Cervicography] for Uterine Cervical Cancer
- The Usefulness of Cervicovaginal Cytology as a Primary Screening Test
- Comparison of human papillomavirus DNA polymerase chain reaction with cervical cytology as a screening test for the detection of cervical intraepithelial neoplasia
- New insights into cervical cancer screening
- A Clinical Effectiveness of Cytology and HPV DNA test (Hybrid capture I) in Cervical Cancer Screening
