Colonic Intramucosal Cancer in the Interposed Colon Treated with Endoscopic Mucosal Resection: A Case Report and Review of Literature
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Department of Gastroenterology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. jsbyeon@amc.seoul.kr
- KMID: 2455637
- DOI: http://doi.org/10.5946/ce.2018.129
Abstract
- Colon interposition is a surgical procedure used for maintenance of luminal conduit after esophagectomy. Although epithelial neoplasia, such as adenoma and adenocarcinoma, may develop in the interposed colon, there are only few case reports on the condition. Due to the rarity of this condition, there is no definite consensus on recommending screening endoscopy for the early detection of neoplasia in the interposed colons. Here, we report a case of intramucosal adenocarcinoma in an interposed colon. Initial endoscopic resection for this tumor failed to accomplish complete resection. A subsequent endoscopic resection was performed 1 month later and complete resection was achieved. Based on our experience and recommendation on screening endoscopy for gastric cancer in Korea, we suggest that regular screening esophagogastroduodenoscopies should be performed following esophagectomy to detect early neoplasia in the stomach and interposed colon and avoid adverse results induced by delayed detection.
MeSH Terms
Figure
-

Fig. 1. Esophagogastroduodenoscopy performed at another hospital. (A) Endoscopic image showing a 20-mm sessile polyp in the interposed colon. (B, C) Endoscopic resection was attempted and piecemeal resection was performed. (D) Complete resection was not achieved, and the remnant residual lesion is visible.
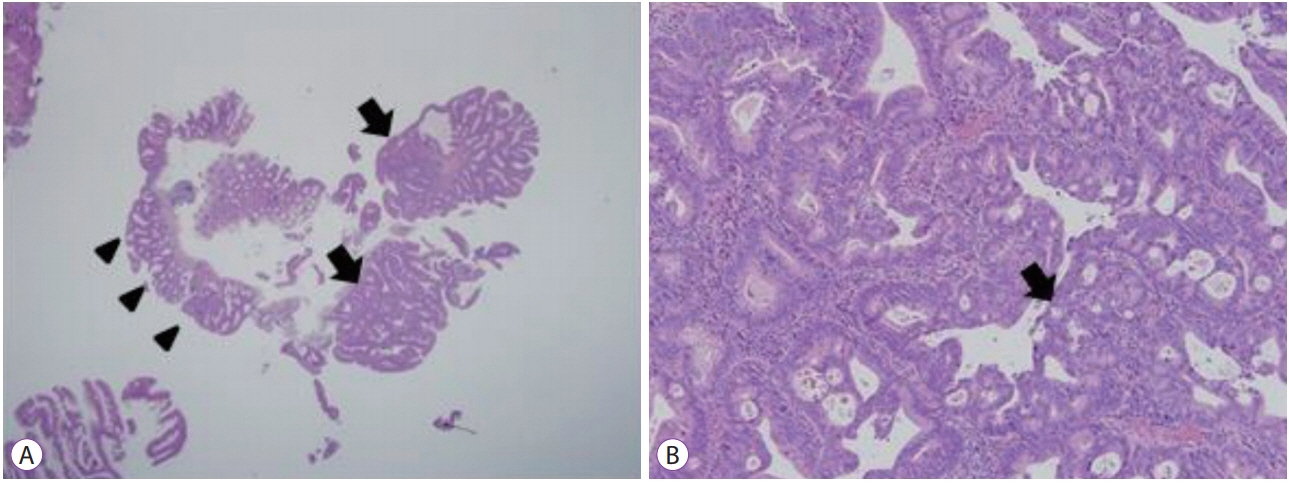
Fig. 2. Histological examination of the endoscopically resected specimen (Hematoxylin and eosin stain). (A) A very low-power scan view image (×12.5) showing simple crypt-like dysplastic glands (arrowheads), a characteristic of villotubular adenoma. The complicated glandular structure suggests adenocarcinomatous changes (arrows). (B) A low-power field view image (×100) showing cribriform formation and back-to-back appearance of a glandular structure with loss of polarity (arrow), suggesting adenocarcinoma.
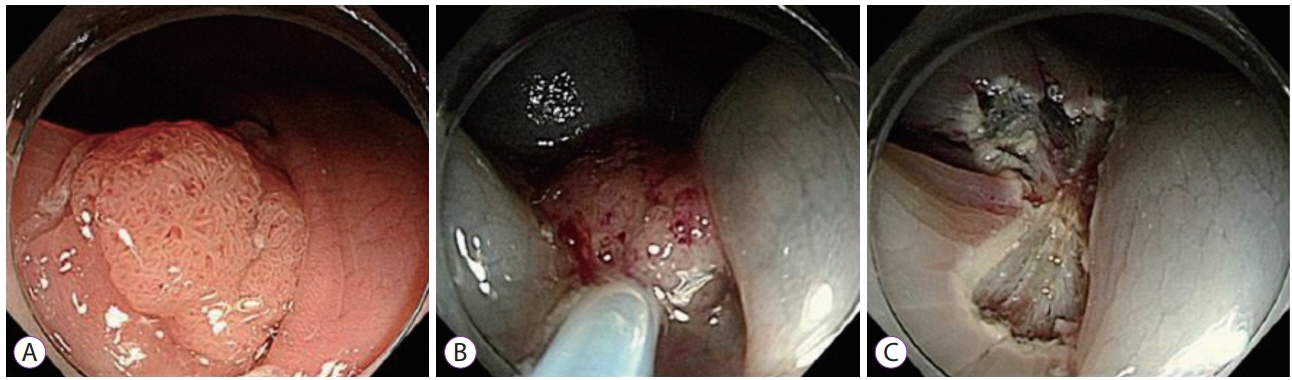
Fig. 3. Repeated endoscopic resection of residual colonic neoplasia at the interposed colon. (A) White light endoscopic image showing a 12-mm residual polyp in the interposed colon. (B, C) Endoscopic mucosal resection was conducted, and the lesion was completely resected by piecemeal fashion in two pieces. Argon plasma coagulation was also performed to eliminate possible microscopic residual lesions.
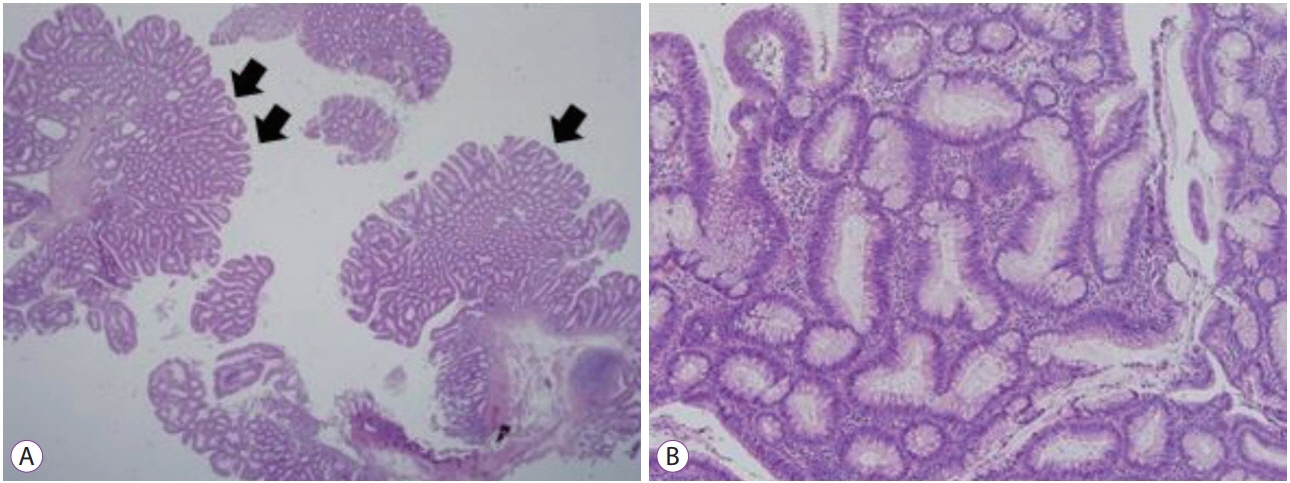
Fig. 4. Histological examination of the specimen resected by repeated endoscopic resection (Hematoxylin and eosin stain). (A) A very low-power scan view (×12.5) showing the typical gross features of the tubular adenoma (arrows). (B) A low-power field view (×100) showing enlarged, hyperchromatic, and elongated nuclei arranged in a stratified configuration along the basement membrane, which is compatible with tubular adenoma.
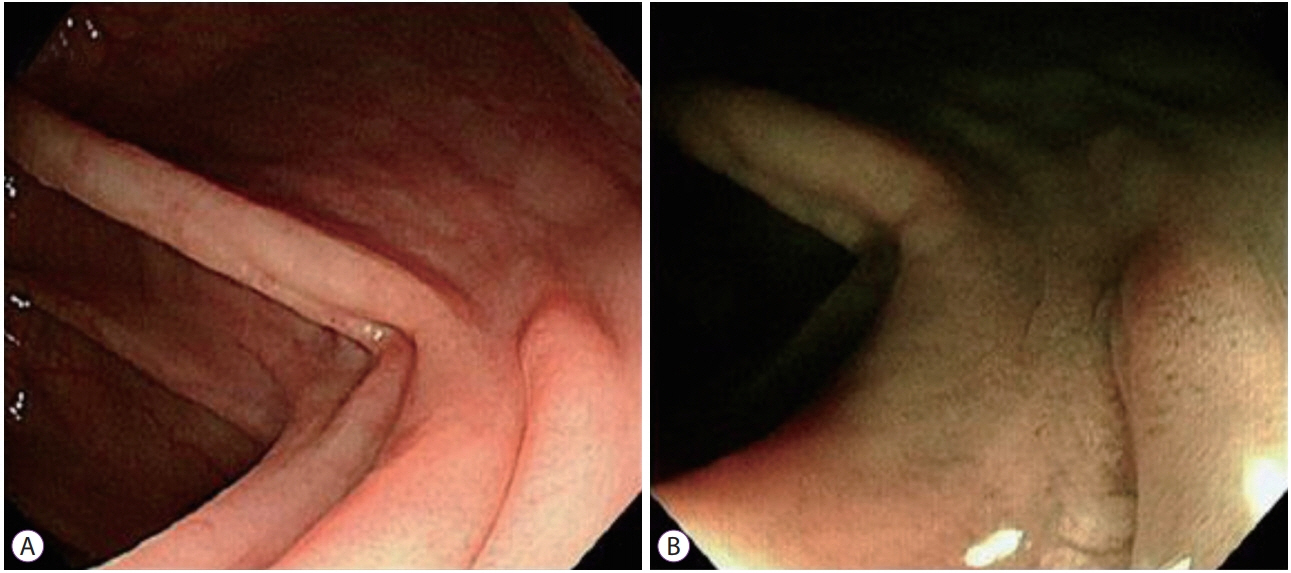
Fig. 5. Follow-up esophagogastroduodenoscopy one year after complete resection of lesion at the interposed colon. A scar was visible at white-light examination (A) and narrow band imaging (B), with no sign of recurrent lesion.
Reference
-
1. Wilkins EW Jr. Long-segment colon substitution for the esophagus. Ann Surg. 1980; 192:722–725.
Article2. Briel JW, Tamhankar AP, Hagen JA, et al. Prevalence and risk factors for ischemia, leak, and stricture of esophageal anastomosis: gastric pull-up versus colon interposition. J Am Coll Surg. 2004; 198:536–541. discussion 541-542.3. Lee K, Kim HR, Park SI, Kim DK, Kim YH, Choi SH. Surgical outcome of colon interposition in esophageal cancer surgery: analysis of risk factors for conduit-related morbidity. Thorac Cardiovasc Surg. 2018; 66:384–389.
Article4. DeMeester SR. Colonic interposition for benign fisease. Oper Tech Thorac Cardiovasc Surg. 2006; 11:232–249.5. Fenoglio CM, Kaye GI, Lane N. Distribution of human colonic lymphatics in normal, hyperplastic, and adenomatous tissue. Its relationship to metastasis from small carcinomas in pedunculated adenomas, with two case reports. Gastroenterology. 1973; 64:51–66.6. Ko OB, Byeon JS, Kim MJ, et al. Clinical outcomes of colonic mucosal cancers with histologically positive or uncertain resection margin after endoscopic resection. Hepatogastroenterology. 2014; 61:65–69.7. Regula J, Wronska E, Polkowski M, et al. Argon plasma coagulation after piecemeal polypectomy of sessile colorectal adenomas: long-term follow-up study. Endoscopy. 2003; 35:212–218.
Article8. Tsiamoulos ZP, Bourikas LA, Saunders BP. Endoscopic mucosal ablation: a new argon plasma coagulation/injection technique to assist complete resection of recurrent, fibrotic colon polyps (with video). Gastrointest Endosc. 2012; 75:400–404.
Article9. Lee BI, Hong SP, Kim SE, et al. Korean guidelines for colorectal cancer screening and polyp detection. Clin Endosc. 2012; 45:25–43.
Article10. Cairns SR, Scholefield JH, Steele RJ, et al. Guidelines for colorectal cancer screening and surveillance in moderate and high risk groups (update from 2002). Gut. 2010; 59:666–689.
Article11. Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012; 143:844–857.
Article12. Goldsmith HS, Beattie EJ Jr. Malignant villous tumor in a colon bypass. Ann Surg. 1968; 167:98–100.
Article13. Hwang HJ, Song KH, Youn YH, et al. A case of more abundant and dysplastic adenomas in the interposed colon than in the native colon. Yonsei Med J. 2007; 48:1075–1078.
Article14. Lee S, Kim ES, Chung WJ, et al. A case of colon cancer developing at the interposed graft for treatment of benign esophageal stricture. Keimyung Medical Journal. 2010; 29:138–142.15. Kim ES, Park KS, Cho KB, Kim MJ. Adenocarcinoma occurring at the interposed colon graft for treatment of benign esophageal stricture. Dis Esophagus. 2012; 25:175.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of More Abundant and Dysplastic Adenomas in the Interposed Colon than in the Native Colon
- Successful Endoscopic Resection of Residual Colonic Mucosa-Associated Lymphoid Tissue Lymphoma after Polypectomy
- Underwater Endoscopic Mucosal Resection without Submucosal Injection Facilitates En bloc Resection of Colon Adenomas Extending into a Diverticulum
- Endoscopic Resection of Undifferentiated Early Gastric Cancer
- Unusual Local Recurrence with Distant Metastasis after Successful Endoscopic Submucosal Dissection for Colorectal Mucosal Cancer
