Comparison of Posterior Capsule Rupture Rate during Phacoemulsification by Novice Ophthalmologists: Microscope vs. Intracameral Illumination
- Affiliations
-
- 1Department of Ophthalmology, Gachon University Gil Hospital, Incheon, Korea. eyedawns@gilhospital.com
- 2DMC Good Eye Clinic, Seoul, Korea.
- 3Department of Ophthalmology, Korea University Guro Hospital, Seoul, Korea.
- 4Department of Ophthalmology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Department of Ophthalmology, Soonchunhyang University Seoul Hospital, Seoul, Korea.
- 6Department of Ophthalmology, Seoul National University Bundang Hospital, Seongnam, Korea.
- KMID: 2453016
- DOI: http://doi.org/10.3341/jkos.2019.60.7.654
Abstract
- PURPOSE
We compared the posterior capsule rupture (PCR) rate between microscope versus intracameral illumination in phacoemulsification surgery performed by novice ophthalmologists.
METHODS
We conducted a retrospective chart review of 300 eyes of 211 patients who underwent phacoemulsification by novice ophthalmologists from March 2012 to October 2017. Novice ophthalmologists (n = 6) were divided into those using microscope illumination (n = 4) and intracameral illumination users (n = 2). The first 50 cataract surgery cases of each novice ophthalmologist were reviewed. The results using a phacoemulsification machine and microscopy were the same. The intraoperative complications and learning curve in each case were evaluated.
RESULTS
Phacoemulsifications performed by novice ophthalmologists showed a statistically significant difference in PCR rate between the microscope illumination (19.0%, 38/200) and intracameral illumination (4.0%, 4/100) groups (p = 0.001). The incidence of PCR was reduced to 22%, 18%, 16%, 12%, and 8% per 10 cases in the microscope group, while it was 15% in the first 10 cases and 0% in 50 cases thereafter in the intracameral illumination group.
CONCLUSIONS
Novice surgeons had a lower PCR rate during cataract surgery using intracameral illumination than using microscope illumination. Both groups showed a tendency for the PCR to decrease with increasing surgical cases, but the intracameral illumination group showed a shorter learning curve.
Keyword
MeSH Terms
Figure
-
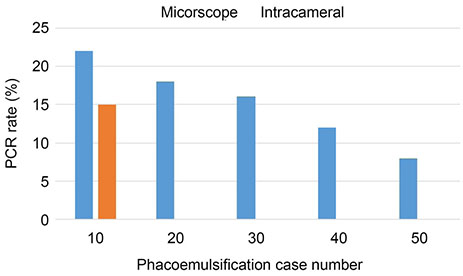
Figure 1 Phacoemulsification learning curve of each illumination. The incidence of posterior capsule rupture was reduced to 22%, 18%, 16%, 12%, and 8% per 10 cases in the microscope group, while 15% in the first 10 cases and 0% in 40 cases thereafter in the intracameral illumination group. PCR = posterior capsule rupture.

Figure 2 Microscope illumination (A) vs. intracameral illumination (B). In microscope illumination, a red reflex is produced by reflection of bright coaxial light from the macula back to the observer (the ocular of an operating microscope). In Intracameral illumination, on the other hand, a side light of intracameral illumination is shining into not macula but peripheral retina. Therefore, the light reflection from the macula back to the observer is decreased. Furthermore, intracameral illumination improved visibility of the lens and enhanced depth perception of the surgical field.
Reference
-
1. Low SA, Braga-Mele R, Yan DB, El-Defrawy S. Intraoperative complication rates in cataract surgery performed by ophthalmology resident trainees compared to staff surgeons in a Canadian academic center. J Cataract Refract Surg. 2018; 44:1344–1349.
Article2. Bhagat N, Nissirios N, Potdevin L, et al. Complications in resident-performed phacoemulsification cataract surgery at new jersey medical school. Br J Ophthalmol. 2007; 91:1315–1317.
Article3. Le K, Bursztyn L, Rootman D, Harissi-Dagher M. National survey of Canadian ophthalmology residency education. Can J Ophthalmol. 2016; 51:219–225.
Article4. Eom Y, Kang SY, Kim HM, Song JS. A survey report on cataract surgical experiences during ophthalmology residency in Korea. J Korean Ophthalmol Soc. 2011; 52:429–433.
Article5. Randleman JB, Wolfe JD, Woodward M, et al. The resident surgeon phacoemulsification learning curve. Arch ophthalmol. 2007; 125:1215–1219.
Article6. Park UC, Kwon JW, Han YK. Clinical results of posterior capsule ruptures in the first 1,000 phacoemulsification cases. J Korean Ophthalmol Soc. 2005; 46:1270–1275.7. Jun JH, Chang SD. Clinical features of posterior capsule rupture during phacoemulsification performed by novice ophthalmologists. J Korean Ophthalmol Soc. 2014; 55:679–685.
Article8. Pingree MF, Crandall AS, Olson RJ. Cataract surgery complications in 1 year at an academic institution. J Cataract Refract Surg. 1999; 25:705–708.
Article9. Seo H, Nam DH, Lee JY, et al. Macular photostress and visual experience between microscope and intracameral illumination during cataract surgery. J Cataract Refract Surg. 2018; 44:190–197.
Article10. Wi J, Seo H, Lee JY, Nam DH. Phacoemulsification using a chisel-shaped illuminator: enhanced depth trench, one-shot crack, and phaco cut. Eur J Ophthalmol. 2016; 26:279–280.
Article11. Moon H, Lee JH, Lee JY, et al. Intracameral dynamic spotlight-assisted cataract surgery in eyes with corneal opacity, small pupil or advanced cataract. Acta Ophthalmol. 2015; 93:388–390.
Article12. Jung Y, Kim IN, Yoon J, et al. Intracameral illuminator-assisted advanced cataract surgery combined with 23-gauge vitrectomy in eyes with poor red reflex. J Cataract Refract Surg. 2013; 39:845–850.
Article13. Lee JY, Yoon J, Kim IN, et al. Intracameral illuminator-guided advanced lens capsule polishing during cataract surgery in eyes with diabetic retinopathy. Retina. 2012; 32:1420–1423.
Article14. Park YM, Park JY, Lee JS, et al. Comparative analysis of brilliant blue G and an intracameral illuminator in assisting visualization of the anterior capsule in eyes with vitreous hemorrhage. J Cataract Refract Surg. 2016; 42:1015–1021.
Article15. Yepez JB, Murati FA, García F, et al. Phacoemulsification outcomes with different illumination techniques. Eur J Ophthalmol. 2017; 27:797–800.
Article16. Rogers GM, Oetting TA, Lee AG, et al. Impact of a structured surgical curriculum on ophthalmic resident cataract surgery complication rates. J Cataract Refract Surg. 2009; 35:1956–1960.
Article17. Allinson RW, Metrikin DC, Fante RG. Incidence of vitreous loss among third-year residents performing phacoemulsification. Ophthalmology. 1992; 99:726–730.
Article18. Ezra DG, Aggarwal R, Michaelides M, et al. Skills acquisition and assessment after a microsurgical skills course for ophthalmology residents. Ophthalmology. 2009; 116:257–262.
Article19. Young BK, Greenberg PB. Is virtual reality training for resident cataract surgeons cost effective? Graefes Arch Clin Exp Ophthalmol. 2013; 251:2295–2296.
Article20. Ramani S, Pradeep TG, Sundaresh DD. Effect of wetlaboratory training on resident performed manual smallincision cataract surgery. Indian J Ophthalmol. 2018; 66:793–797.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Features of Posterior Capsule Rupture during Phacoemulsification Performed by Novice Ophthalmologists
- A Case of Isolated Posterior Capsule Rupture Caused by Blunt Ocular Trauma
- Analysis of Cause and Outcome of Posterior Capsular Rupture during Phacoemulsification in Cataract Surgery
- Cost-Effectiveness Analysis of Cataract Surgery for the Beginners Using Intraocular Illumination
- Effect of Intracameral Triamcinolone to Control Inflammation in Rabbit Eyes
