Extended Use of Extracorporeal Membrane Oxygenation for Acute Respiratory Distress Syndrome: A Retrospective Multicenter Study
- Affiliations
-
- 1Division of Pulmonary, Allergy and Critical Care Medicine, Department of Internal Medicine, Pusan National University, School of Medicine, Busan, Korea.
- 2Department of Internal Medicine, Chonbuk National University Medical School, Jeonju, Korea.
- 3Department of Clinical Epidemiology and Biostatistics, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 4Department of Pulmonary, Allergy, and Critical Care Medicine, Hallym University Dongtan Sacred Heart Hospital, Hwaseong, Korea.
- 5Department of Critical Care Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 6Department of Pulmonary and Critical Care Medicine, Kyung Hee University Hospital at Gangdong, Kyung Hee University School of Medicine, Seoul, Korea.
- 7Department of Internal Medicine, Ulsan University Hospital, University of Ulsan College of Medicine, Ulsan, Korea.
- 8Division of Pulmonology and Critical Care Medicine, Dongguk University Ilsan Hospital, Dongguk University College of Medicine, Goyang, Korea.
- 9Department of Pulmonology and Critical Care Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea.
- 10Division of Pulmonary and Critical Care Medicine, Department of Medicine, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea.
- 11Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea.
- 12Division of Pulmonary and Critical Care Medicine, Department of Medicine, Hallym University Sacred Heart Hospital, Anyang, Korea.
- 13Department of Internal Medicine, CHA Bundang Medical Center, CHA University School of Medicine, Seongnam, Korea.
- 14Department of Pulmonary and Critical Care Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. sbhong@amc.seoul.kr
- KMID: 2450903
- DOI: http://doi.org/10.4046/trd.2018.0061
Abstract
- BACKGROUND
Beyond its current function as a rescue therapy in acute respiratory distress syndrome (ARDS), extracorporeal membrane oxygenation (ECMO) may be applied in ARDS patients with less severe hypoxemia to facilitate lung protective ventilation. The purpose of this study was to evaluate the efficacy of extended ECMO use in ARDS patients.
METHODS
This study reviewed 223 adult patients who had been admitted to the intensive care units of 11 hospitals in Korea and subsequently treated using ECMO. Among them, the 62 who required ECMO for ARDS were analyzed. The patients were divided into two groups according to pre-ECMO arterial blood gas: an extended group (n=14) and a conventional group (n=48).
RESULTS
Baseline characteristics were not different between the groups. The median arterial carbon dioxide tension/fraction of inspired oxygen (FiO2) ratio was higher (97 vs. 61, p<0.001) while the median FiO2 was lower (0.8 vs. 1.0, p<0.001) in the extended compared to the conventional group. The 60-day mortality was 21% in the extended group and 54% in the conventional group (p=0.03). Multivariate analysis indicated that the extended use of ECMO was independently associated with reduced 60-day mortality (odds ratio, 0.10; 95% confidence interval, 0.02-0.64; p=0.02). Lower median peak inspiratory pressure and median dynamic driving pressure were observed in the extended group 24 hours after ECMO support.
CONCLUSION
Extended indications of ECMO implementation coupled with protective ventilator settings may improve the clinical outcome of patients with ARDS.
Keyword
MeSH Terms
Figure
-

Figure 1 Illustration of a study flow diagram. ECMO: extracorporeal membrane oxygenation; BTT: bridge to transplant; VA: venoarterial; COPD: chronic obstructive pulmonary disease; ILD: interstitial lung disease; ARDS: acute respiratory distress syndrome.

Figure 2 Kaplan–Meier survival curves of the patients under study. ECMO: extracorporeal membrane oxygenation.
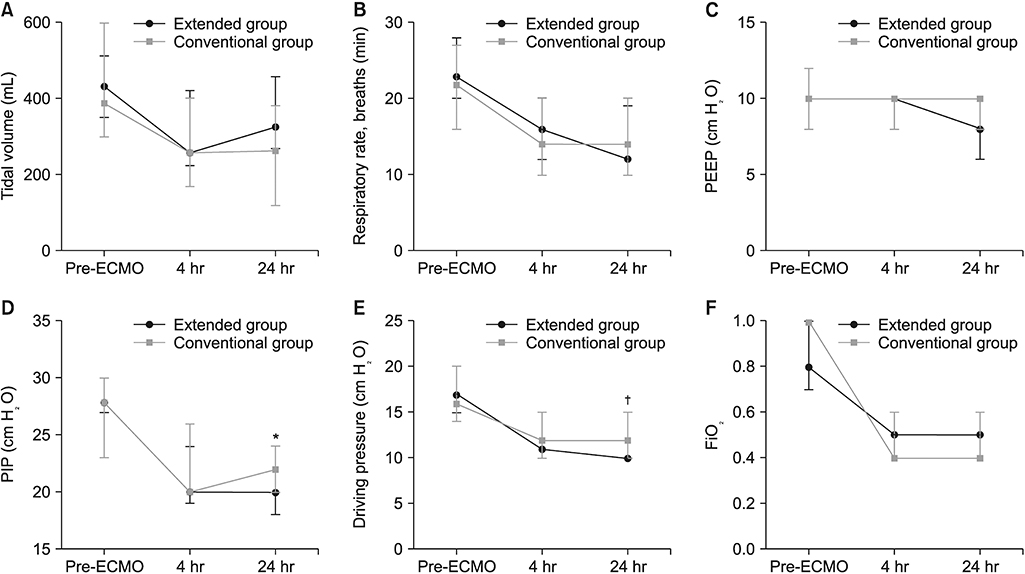
Figure 3 Serial changes in tidal volume (A), respiratory rate (B), positive end-expiratory pressure (PEEP) (C), peak inspiratory pressure (PIP) (D), dynamic driving pressure (E), and fraction of inspired oxygen (FiO2) (F) in the extended group (dark line) and the conventional group (gray line) during the 24-hour study period. Data is presented as a median value (interquartile range). *p<0.05. †p=0.13. ECMO: extracorporeal membrane oxygenation.
Reference
-
1. Ware LB, Matthay MA. The acute respiratory distress syndrome. N Engl J Med. 2000; 342:1334–1349.
Article2. ARDS Definition Task Force. Ranieri VM, Rubenfeld GD, Thompson BT, Ferguson ND, Caldwell E, et al. Acute respiratory distress syndrome: the Berlin definition. JAMA. 2012; 307:2526–2533.3. Peek GJ, Mugford M, Tiruvoipati R, Wilson A, Allen E, Thalanany MM, et al. Efficacy and economic assessment of conventional ventilatory support versus extracorporeal membrane oxygenation for severe adult respiratory failure (CESAR): a multicentre randomised controlled trial. Lancet. 2009; 374:1351–1363.
Article4. Villar J, Blanco J, Anon JM, Santos-Bouza A, Blanch L, Ambros A, et al. The ALIEN study: incidence and outcome of acute respiratory distress syndrome in the era of lung protective ventilation. Intensive Care Med. 2011; 37:1932–1941.
Article5. Slutsky AS, Ranieri VM. Ventilator-induced lung injury. N Engl J Med. 2013; 369:2126–2136.
Article6. Acute Respiratory Distress Syndrome Network. Brower RG, Matthay MA, Morris A, Schoenfeld D, Thompson BT, et al. Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. N Engl J Med. 2000; 342:1301–1308.
Article7. Briel M, Meade M, Mercat A, Brower RG, Talmor D, Walter SD, et al. Higher vs lower positive end-expiratory pressure in patients with acute lung injury and acute respiratory distress syndrome: systematic review and meta-analysis. JAMA. 2010; 303:865–873.8. Australia and New Zealand Extracorporeal Membrane Oxygenation (ANZ ECMO) Influenza Investigators. Davies A, Jones D, Bailey M, Beca J, Bellomo R, et al. Extracorporeal membrane oxygenation for 2009 influenza A (H1N1) acute respiratory distress syndrome. JAMA. 2009; 302:1888–1895.9. Pham T, Combes A, Roze H, Chevret S, Mercat A, Roch A, et al. Extracorporeal membrane oxygenation for pandemic influenza A(H1N1)-induced acute respiratory distress syndrome: a cohort study and propensity-matched analysis. Am J Respir Crit Care Med. 2013; 187:276–285.10. Brodie D, Bacchetta M. Extracorporeal membrane oxygenation for ARDS in adults. N Engl J Med. 2011; 365:1905–1914.
Article11. Hager DN, Krishnan JA, Hayden DL, Brower RG. ARDS Clinical Trials Network. Tidal volume reduction in patients with acute lung injury when plateau pressures are not high. Am J Respir Crit Care Med. 2005; 172:1241–1245.
Article12. Terragni PP, Rosboch G, Tealdi A, Corno E, Menaldo E, Davini O, et al. Tidal hyperinflation during low tidal volume ventilation in acute respiratory distress syndrome. Am J Respir Crit Care Med. 2007; 175:160–166.
Article13. Knaus WA, Draper EA, Wagner DP, Zimmerman JE. APACHE II: a severity of disease classification system. Crit Care Med. 1985; 13:818–829.14. Vincent JL, Moreno R, Takala J, Willatts S, De Mendonca A, Bruining H, et al. The SOFA (Sepsis-related Organ Failure Assessment) score to describe organ dysfunction/failure. On behalf of the Working Group on Sepsis-Related Problems of the European Society of Intensive Care Medicine. Intensive Care Med. 1996; 22:707–710.15. Schmidt M, Zogheib E, Roze H, Repesse X, Lebreton G, Luyt CE, et al. The PRESERVE mortality risk score and analysis of long-term outcomes after extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. Intensive Care Med. 2013; 39:1704–1713.
Article16. Schmidt M, Bailey M, Sheldrake J, Hodgson C, Aubron C, Rycus PT, et al. Predicting survival after extracorporeal membrane oxygenation for severe acute respiratory failure. The Respiratory Extracorporeal Membrane Oxygenation Survival Prediction (RESP) score. Am J Respir Crit Care Med. 2014; 189:1374–1382.
Article17. Chiu LC, Hu HC, Hung CY, Chang CH, Tsai FC, Yang CT, et al. Dynamic driving pressure associated mortality in acute respiratory distress syndrome with extracorporeal membrane oxygenation. Ann Intensive Care. 2017; 7:12.
Article18. Bellani G, Laffey JG, Pham T, Fan E, Brochard L, Esteban A, et al. Epidemiology, patterns of care, and mortality for patients with acute respiratory distress syndrome in intensive care units in 50 countries. JAMA. 2016; 315:788–800.
Article19. Bein T, Grasso S, Moerer O, Quintel M, Guerin C, Deja M, et al. The standard of care of patients with ARDS: ventilatory settings and rescue therapies for refractory hypoxemia. Intensive Care Med. 2016; 42:699–711.
Article20. Combes A, Hajage D, Capellier G, Demoule A, Lavoue S, Guervilly C, et al. Extracorporeal membrane oxygenation for severe acute respiratory distress syndrome. N Engl J Med. 2018; 378:1965–1975.
Article21. Bein T, Weber-Carstens S, Goldmann A, Muller T, Staudinger T, Brederlau J, et al. Lower tidal volume strategy (approximately 3 ml/kg) combined with extracorporeal CO2 removal versus ‘conventional’ protective ventilation (6 ml/kg) in severe ARDS: the prospective randomized Xtravent-study. Intensive Care Med. 2013; 39:847–856.22. Serpa Neto A, Schmidt M, Azevedo LC, Bein T, Brochard L, Beutel G, et al. Associations between ventilator settings during extracorporeal membrane oxygenation for refractory hypoxemia and outcome in patients with acute respiratory distress syndrome: a pooled individual patient data analysis: mechanical ventilation during ECMO. Intensive Care Med. 2016; 42:1672–1684.23. Schmidt GA. Cardiopulmonary interactions in acute lung injury. Curr Opin Crit Care. 2013; 19:51–56.
Article24. MacLaren G, Combes A, Bartlett RH. Contemporary extracorporeal membrane oxygenation for adult respiratory failure: life support in the new era. Intensive Care Med. 2012; 38:210–220.
Article25. Rehder KJ, Turner DA, Hartwig MG, Williford WL, Bonadonna D, Walczak RJ Jr, et al. Active rehabilitation during extracorporeal membrane oxygenation as a bridge to lung transplantation. Respir Care. 2013; 58:1291–1298.
Article26. Hodgson CL, Fan E. A step up for extracorporeal membrane oxygenation: active rehabilitation. Respir Care. 2013; 58:1388–1390.
Article27. Herridge MS, Cheung AM, Tansey CM, Matte-Martyn A, Diaz-Granados N, Al-Saidi F, et al. One-year outcomes in survivors of the acute respiratory distress syndrome. N Engl J Med. 2003; 348:683–693.
Article28. Schmidt M, Stewart C, Bailey M, Nieszkowska A, Kelly J, Murphy L, et al. Mechanical ventilation management during extracorporeal membrane oxygenation for acute respiratory distress syndrome: a retrospective international multicenter study. Crit Care Med. 2015; 43:654–664.29. Balzer F, Menk M, Ziegler J, Pille C, Wernecke KD, Spies C, et al. Predictors of survival in critically ill patients with acute respiratory distress syndrome (ARDS): an observational study. BMC Anesthesiol. 2016; 16:108.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Treatment of acute respiratory failure: extracorporeal membrane oxygenation
- Successful use of extracorporeal membrane oxygenation for sudden aggravation of acute respiratory distress syndrome: A case report
- Recovery from Acute Respiratory Distress Syndrome with Long-Run Extracorporeal Membrane Oxygenation
- The Treatment of Adult Respiratory Distress Syndrome (ARDS) Using Extracorporeal Membrane Oxygenation (ECMO)
- Extracorporeal Membrane Oxygenation for Complicated Scrub Typhus
