Infect Chemother.
2019 Jun;51(2):142-149. 10.3947/ic.2019.51.2.142.
Thromboembolism in Mycobacterium tuberculosis Infection: Analysis and Literature Review
- Affiliations
-
- 1Division of Hematology and Medical Oncology, Department of Internal medicine, Seoul National University Hospital, Seoul, Korea.
- 2Division of Hematology and Medical Oncology, Department of Internal medicine, The Catholic University of Korea, Incheon St. Mary's Hospital, Incheon, Korea.
- 3Division of Hematology and Medical Oncology, Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul, Korea. floresta405@gamil.com
- 4Division of Pulmonology, Department of Internal Medicine, Seoul National University Boramae Medical Center, Seoul, Korea.
- 5Department of Internal Medicine, Veterans Health Service Medical Center, Seoul, Korea.
- KMID: 2450870
- DOI: http://doi.org/10.3947/ic.2019.51.2.142
Abstract
- BACKGROUND
Tuberculosis is associated with hypercoagulation; however, there are few reports of cases thromboembolism and tuberculosis at the same time in the real world. The purpose of this study was to report the incidence and clinical course of thromboembolism in patients diagnosed with tuberculosis.
MATERIALS AND METHODS
We retrospectively analyzed the data of patients who were diagnosed with both tuberculosis and thromboembolism including pulmonary thromboembolism (PTE) or deep vein thrombosis (DVT) at Seoul National University Boramae Medical Center from January 2000 through March 2015.
RESULTS
Among the 7905 tuberculosis patients, 49 (0.6%) exhibited PTE, DVT, or both at or after the time of tuberculosis diagnosis. All patients treated for tuberculosis started with isoniazid, ethambutol, rifampicin, and pyrazinamide. Eight patients were switched to treatment with second-line medication because of resistance or adverse events. About half of the patients (n = 21, 44.7%) had thrombosis at the time of tuberculosis diagnosis. Of 48 patients treated for thromboembolism, 36 received warfarin. A total of 20 patients improved symptom caused by thrombosis, and 10 patients were confirmed cure by image study such as computed tomography or doppler ultrasonography. Eight patients who were treated with warfarin had persistent thrombosis. Five patients (10.2%) experienced major bleeding that required hospitalization. All of these bleeding events were associated with warfarin therapy.
CONCLUSIONS
Careful attention to PTE/DVT is needed at the time of diagnosis of tuberculosis and during anti-tuberculosis therapy. Warfarin therapy administered with anti-tuberculosis medication requires frequent monitoring to prevent major bleeding.
MeSH Terms
-
Diagnosis
Ethambutol
Hemorrhage
Hospitalization
Humans
Incidence
Isoniazid
Mycobacterium tuberculosis*
Mycobacterium*
Pulmonary Embolism
Pyrazinamide
Retrospective Studies
Rifampin
Seoul
Thromboembolism*
Thrombosis
Tuberculosis
Ultrasonography, Doppler
Venous Thrombosis
Warfarin
Ethambutol
Isoniazid
Pyrazinamide
Rifampin
Warfarin
Figure
-
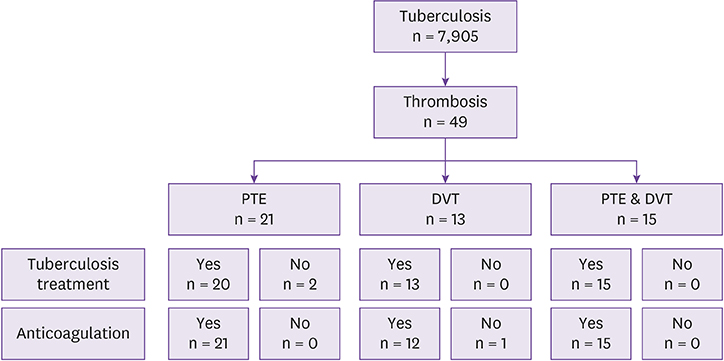
Figure 1 Pulmonary thromboembolism/deep vein thrombosis incidence of tuberculosis and treatment. The incidence of PTE/DVT and treatment pattern of tuberculosis and thromboembolism was visualized in this figure. PTE, pulmonary thromboembolism; DVT, deep vein thrombosis.
Reference
-
1. World Health Organization (WHO). Global tuberculosis report 2015, 20th ed. Accessed 27 March 2017. Available at: http://www.who.int/iris/handle/10665/191102.2. Ben Amar J, Dahri B, Aouina H, Bouacha H. [Venous thromboembolism in patients with acute tuberculosis]. Rev Pneumol Clin. 2015; 71:327–334.3. Lee CR, Thrasher KA. Difficulties in anticoagulation management during coadministration of warfarin and rifampin. Pharmacotherapy. 2001; 21:1240–1246.
Article4. Naithani R, Agrawal N, Choudhary VP. Deep venous thrombosis associated with tuberculosis. Blood Coagul Fibrinolysis. 2007; 18:377–380.
Article5. El Fekih L, Oueslati I, Hassene H, Fenniche S, Belhabib D, Megdiche ML. Association deep veinous thrombosis with pulmonary tuberculosis. Tunis Med. 2009; 87:328–329.6. Goncalves IM, Alves DC, Carvalho A, do Ceu Brito M, Calvario F, Duarte R. Tuberculosis and venous thromboembolism: a case series. Cases J. 2009; 2:9333.
Article7. Silverstein M, Heit JA, Mohr DN, Petterson TM, O'Fallon WM, Melton LJ 3rd. Trends in the incidence of deep vein thrombosis and pulmonary embolism: a 25-year population-based study. Arch Intern Med. 1998; 158:585–593.
Article8. Esmon CT. The interactions between inflammation and coagulation. Br J Haematol. 2005; 131:417–430.
Article9. Schultz M, Millo J, Levi M, Hack CE, Weverling GJ, Garrard CS, van der Poll T. Local activation of coagulation and inhibition of fibrinolysis in the lung during ventilator associated pneumonia. Thorax. 2004; 59:130–135.
Article10. Günther A, Mosavi P, Heinemann S, Ruppert C, Muth H, Markart P, Grimminger F, Walmrath D, Temmesfeld-Wollbrück B, Seeger W. Alveolar fibrin formation caused by enhanced procoagulant and depressed fibrinolytic capacities in severe pneumonia. comparison with the acute respiratory distress. Am J Respir Crit Care Med. 2000; 161:454–462.
Article11. Robson S, White NW, Aronson I, Woollgar R, Goodman H, Jacobs P. Acute-phase response and the hypercoagulable state in pulmonary tuberculosis. Br J Haematol. 1996; 93:943–949.
Article12. Kager LM, Blok DC, Lede IO, Rahman W, Afroz R, Bresser P, van der Zee JS, Ghose A, Visser CE, de Jong MD, Tanck MW, Zahed AS, Alam KM, Hassan M, Hossain A, Lutter R, Veer CV, Dondorp AM, Meijers JC, van der Poll T. Pulmonary tuberculosis induces a systemic hypercoagulable state. J Infect. 2015; 70:323–334.
Article13. Turken O, Kunter E, Sezer M, Solmazgul E, Cerrahoglu K, Bozkanat E, Ozturk A, Ilvan A. Hemostatic changes in active pulmonary tuberculosis. Int J Tuberc Lung Dis. 2002; 6:927–932.14. World Health Organization (WHO). Treatment of tuberculosis: guidelines, 4th edition. Accessed 27 March 2017. Available at: http://www.who.int/iris/handle/10665/44165.15. White NW. Venous thrombosis and rifampicin. Lancet. 1989; 2:434–435.
Article16. van Es N, Coppens M, Schulman S, Middeldorp S, Büller HR. Direct oral anticoagulants compared with vitamin K antagonists for acute venous thromboembolism: evidence from phase 3 trials. Blood. 2014; 124:1968–1975.
Article17. Konstantinides SV, Barco S, Lankeit M, Meyer G. Management of pulmonary embolism: an update. J Am Coll Cardiol. 2016; 67:976–990.18. Lee CR, Thrasher KA. Difficulties in anticoagulation management during coadministration of warfarin and rifampin. Pharmacotherapy. 2001; 21:1240–1246.
Article19. Martins MA, Reis AM, Sales MF, Nobre V, Ribeiro DD, Rocha MO, Ribeiro AL. Rifampicin-warfarin interaction leading to macroscopic hematuria: a case report and review of the literature. BMC Pharmacol Toxicol. 2013; 14:27.
Article20. Anderson FA Jr, Spencer FA. Risk factors for venous thromboembolism. Circulation. 2003; 107:23 Suppl 1. I9–I16.
Article21. Anderson FA, Wheeler HB, Goldberg RJ, Hosmer DW, Forcier A. The prevalence of risk factors for venous thromboembolism among hospital patients. Arch Intern Med. 1992; 152:1660–1664.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Differentiation between Mycobacterium bovis and Mycobacterium tuberculosis Infection
- Lymphomatoid Papulosis with Mycobacterium Other Than Tuberculosis
- Pandemic Influenza (H1N1) and Mycobacterium tuberculosis Co-infection
- Localized Empyema due to Mycobacterium bovis
- A Case of Tuberculosis Verrucosa Cutis with Ulcer in a Patient with Pulmonary Tuberculosis
