Endocrinol Metab.
2019 Jun;34(2):187-194. 10.3803/EnM.2019.34.2.187.
Impaired Cortisol and Growth Hormone Counterregulatory Responses among Severe Hypoglycemic Patients with Type 2 Diabetes Mellitus
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Konkuk University School of Medicine, Seoul, Korea. skh2k@kuh.ac.kr
- 2Division of Endocrinology and Metabolism, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea.
- KMID: 2450519
- DOI: http://doi.org/10.3803/EnM.2019.34.2.187
Abstract
- BACKGROUND
Elevated levels of cortisol and growth hormone are critical counterregulatory responses to severe hypoglycemia. However, the proportion and clinical characteristics of patients with type 2 diabetes mellitus (DM) who fail to show appropriate cortisol and/or growth hormone secretion in response to severe hypoglycemia have not been investigated.
METHODS
We measured plasma cortisol and growth hormone levels in type 2 DM patients with severe hypoglycemia who visited the emergency department between 2006 and 2015.
RESULTS
Of 112 hypoglycemic patients, 23 (20.5%) had an impaired cortisol response (<18 µg/dL) and 82 patients (73.2%) had an impaired growth hormone response (<5 ng/mL). Nineteen patients (17.0%) had impaired responses to both cortisol and growth hormone. The patients with impaired responses of cortisol, growth hormone, and both hormones were significantly older and more likely to be female, and had higher admission rates, lower growth hormone levels, and lower adrenocorticotropic hormone levels than the patients with a normal hormonal response. Multivariate logistic regression analysis indicated that an impaired growth hormone response was significantly associated with advanced age, shorter DM duration, a higher admission rate, and a higher body mass index (BMI). An impaired cortisol response was significantly associated with growth hormone levels. Patients with an impaired growth hormone response had higher admission rates than patients with a normal response.
CONCLUSION
A considerable number of type 2 DM patients had impaired cortisol and/or growth hormone responses to severe hypoglycemia. Advanced age, shorter DM duration, and higher BMI were independently associated with an abnormal growth hormone response.
MeSH Terms
Figure
-
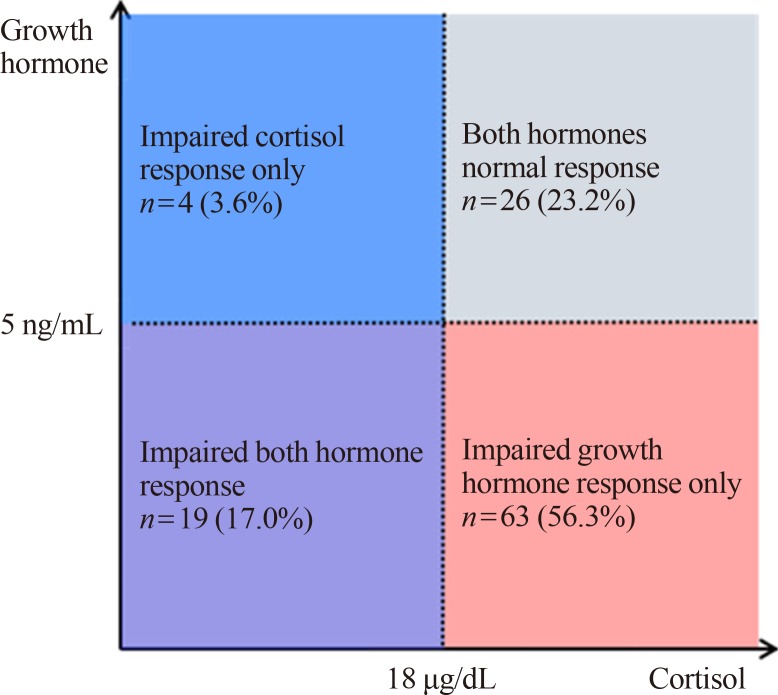
Fig. 1 Number of patients with impaired cortisol and/or growth hormone response during severe hypoglycemia. The impaired cortisol response group includes patients with an impaired cortisol response only (blue box) and those with impaired responses of both hormones (purple box). The impaired growth hormone response group includes patients with an impaired growth hormone response only (red box) and an impaired response of both hormones (purple box).
Reference
-
1. Seaquist ER, Anderson J, Childs B, Cryer P, Dagogo-Jack S, Fish L, et al. Hypoglycemia and diabetes: a report of a workgroup of the American Diabetes Association and the Endocrine Society. Diabetes Care. 2013; 36:1384–1395. PMID: 23589542.
Article2. Desouza CV, Bolli GB, Fonseca V. Hypoglycemia, diabetes, and cardiovascular events. Diabetes Care. 2010; 33:1389–1394. PMID: 20508232.
Article3. Zoungas S, Patel A, Chalmers J, de Galan BE, Li Q, Billot L, et al. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010; 363:1410–1418. PMID: 20925543.
Article4. Yaffe K, Falvey CM, Hamilton N, Harris TB, Simonsick EM, Strotmeyer ES, et al. Association between hypoglycemia and dementia in a biracial cohort of older adults with diabetes mellitus. JAMA Intern Med. 2013; 173:1300–1306. PMID: 23753199.
Article5. Tesfaye N, Seaquist ER. Neuroendocrine responses to hypoglycemia. Ann N Y Acad Sci. 2010; 1212:12–28. PMID: 21039590.
Article6. Cryer PE. Mechanisms of hypoglycemia-associated autonomic failure in diabetes. N Engl J Med. 2013; 369:362–372. PMID: 23883381.
Article7. Rizza RA, Cryer PE, Gerich JE. Role of glucagon, catecholamines, and growth hormone in human glucose counterregulation. Effects of somatostatin and combined alpha- and beta-adrenergic blockade on plasma glucose recovery and glucose flux rates after insulin-induced hypoglycemia. J Clin Invest. 1979; 64:62–71. PMID: 36413.8. Feldman JM, Plonk JW, Bivens CH. The role of cortisol and growth hormone in the counter-regulation of insulin-induced hypoglycemia. Horm Metab Res. 1975; 7:378–381. PMID: 1183916.
Article9. Boyle PJ, Cryer PE. Growth hormone, cortisol, or both are involved in defense against, but are not critical to recovery from, hypoglycemia. Am J Physiol. 1991; 260:E395–E402. PMID: 2003593.
Article10. Schneider HJ, Aimaretti G, Kreitschmann-Andermahr I, Stalla GK, Ghigo E. Hypopituitarism. Lancet. 2007; 369:1461–1470. PMID: 17467517.
Article11. Kargi AY, Merriam GR. Diagnosis and treatment of growth hormone deficiency in adults. Nat Rev Endocrinol. 2013; 9:335–345. PMID: 23629539.
Article12. Charmandari E, Nicolaides NC, Chrousos GP. Adrenal insufficiency. Lancet. 2014; 383:2152–2167. PMID: 24503135.
Article13. Watts AG, Donovan CM. Sweet talk in the brain: glucosensing, neural networks, and hypoglycemic counterregulation. Front Neuroendocrinol. 2010; 31:32–43. PMID: 19836412.
Article14. Davis SN, Shavers C, Mosqueda-Garcia R, Costa F. Effects of differing antecedent hypoglycemia on subsequent counterregulation in normal humans. Diabetes. 1997; 46:1328–1335. PMID: 9231658.
Article15. Heller SR, Cryer PE. Reduced neuroendocrine and symptomatic responses to subsequent hypoglycemia after 1 episode of hypoglycemia in nondiabetic humans. Diabetes. 1991; 40:223–226. PMID: 1991573.
Article16. Davis MR, Shamoon H. Counterregulatory adaptation to recurrent hypoglycemia in normal humans. J Clin Endocrinol Metab. 1991; 73:995–1001. PMID: 1939537.
Article17. Galassetti P, Mann S, Tate D, Neill RA, Costa F, Wasserman DH, et al. Effects of antecedent prolonged exercise on subsequent counterregulatory responses to hypoglycemia. Am J Physiol Endocrinol Metab. 2001; 280:E908–E917. PMID: 11350772.
Article18. Davis SN, Shavers C, Costa F, Mosqueda-Garcia R. Role of cortisol in the pathogenesis of deficient counterregulation after antecedent hypoglycemia in normal humans. J Clin Invest. 1996; 98:680–691. PMID: 8698859.
Article19. McGregor VP, Banarer S, Cryer PE. Elevated endogenous cortisol reduces autonomic neuroendocrine and symptom responses to subsequent hypoglycemia. Am J Physiol Endocrinol Metab. 2002; 282:E770–E777. PMID: 11882496.
Article20. Gustavson SM, Sandoval DA, Ertl AC, Bao S, Raj SR, Davis SN. Stimulation of both type I and type II corticosteroid receptors blunts counterregulatory responses to subsequent hypoglycemia in healthy man. Am J Physiol Endocrinol Metab. 2008; 294:E506–E512. PMID: 18182467.
Article21. Meneilly GS, Cheung E, Tuokko H. Altered responses to hypoglycemia of healthy elderly people. J Clin Endocrinol Metab. 1994; 78:1341–1348. PMID: 8200936.
Article22. Fanelli C, Pampanelli S, Epifano L, Rambotti AM, Ciofetta M, Modarelli F, et al. Relative roles of insulin and hypoglycaemia on induction of neuroendocrine responses to, symptoms of, and deterioration of cognitive function in hypoglycaemia in male and female humans. Diabetologia. 1994; 37:797–807. PMID: 7988782.
Article23. Diamond MP, Hallarman L, Starick-Zych K, Jones TW, Connolly-Howard M, Tamborlane WV, et al. Suppression of counterregulatory hormone response to hypoglycemia by insulin per se. J Clin Endocrinol Metab. 1991; 72:1388–1390. PMID: 2026760.
Article24. Johannsson G, Bjarnason R, Bramnert M, Carlsson LM, Degerblad M, Manhem P, et al. The individual responsiveness to growth hormone (GH) treatment in GH-deficient adults is dependent on the level of GH-binding protein, body mass index, age, and gender. J Clin Endocrinol Metab. 1996; 81:1575–1581. PMID: 8636370.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Hyperglycemic Hyperosmolar Syndrome Induced by Steroid Treatment for Idiopathic Thrombocytopenic Purpura
- Glucose Counterregulatory Hormone Response During Hypoglycemia due to Endogenous Hyperinsulinemia
- Diabetes and Endocrine Disease
- A Case with Empty Sella Syndrome Combined with Multiple Anterior Pituitary Hormone Deficiencies Presenting as Hypoglycemic Coma
- The Effect of Growth Hormone on Carbohydrate Metabolism in Turner Syndrome
