Chronic Cavitary Pulmonary Histoplasmosis in a Non-HIV and Immunocompromised Patient without Overseas Travel History
- Affiliations
-
- 1Division of Infectious Diseases, Department of Internal Medicine, Korea University College of Medicine, Seoul, Korea. cmcws@medimail.co.kr
- 2Department of Pathology, Korea University College of Medicine, Seoul, Korea.
- KMID: 2450367
- DOI: http://doi.org/10.3349/ymj.2015.56.3.871
Abstract
- Korea is not known as an endemic area for Histoplasma. However, we experienced a case of histoplasmosis in a person who had never been abroad. A 65-year-old female was admitted to the hospital for evaluation of multiple lung nodules. A computed tomography (CT) scan of the chest showed multiple ill-defined consolidations and cavitations in all lobes of both lungs. The patient underwent a CT-guided lung biopsy, and a histopathology study showed findings compatible with histoplasmosis. Based on biopsy results and clinical findings, the patient was diagnosed with chronic cavitary pulmonary histoplasmosis. The patient recovered completely following itraconazole treatment. This is the first case report of pulmonary histoplasmosis unconnected with either HIV infection or endemicity in Korea.
MeSH Terms
-
Aged
Antifungal Agents/therapeutic use
Biopsy
Female
Histoplasma/*isolation & purification
Histoplasmosis/*diagnosis/drug therapy/microbiology
Humans
*Immunocompromised Host
Itraconazole/therapeutic use
Lung Diseases, Fungal/*diagnosis/drug therapy
Republic of Korea
Tomography, X-Ray Computed
Treatment Outcome
Antifungal Agents
Itraconazole
Figure
-
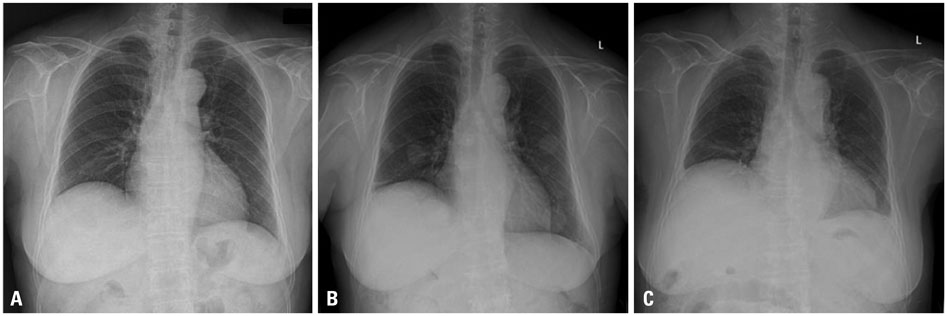
Fig. 1 Chest X-ray images. (A) A chest X-ray taken 6 months before a diagnosis. (B) A chest X-ray taken before the start of treatment shows multiple nodules in both lungs. (C) A chest X-ray taken 12-month after treatment shows complete resolution of the nodules.
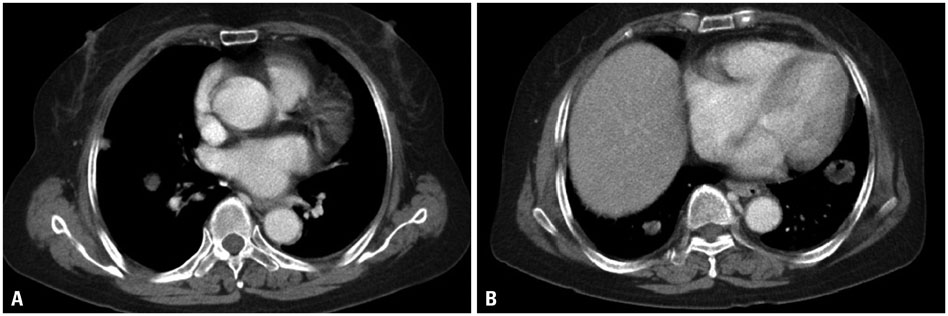
Fig. 2 Chest contrast-enhanced computed tomography (CT) scan images. (A) The chest CT scan shows well-defined multiple nodules of various sizes in both lung fields. (B) Some nodules have low internal attenuation or cavitation.
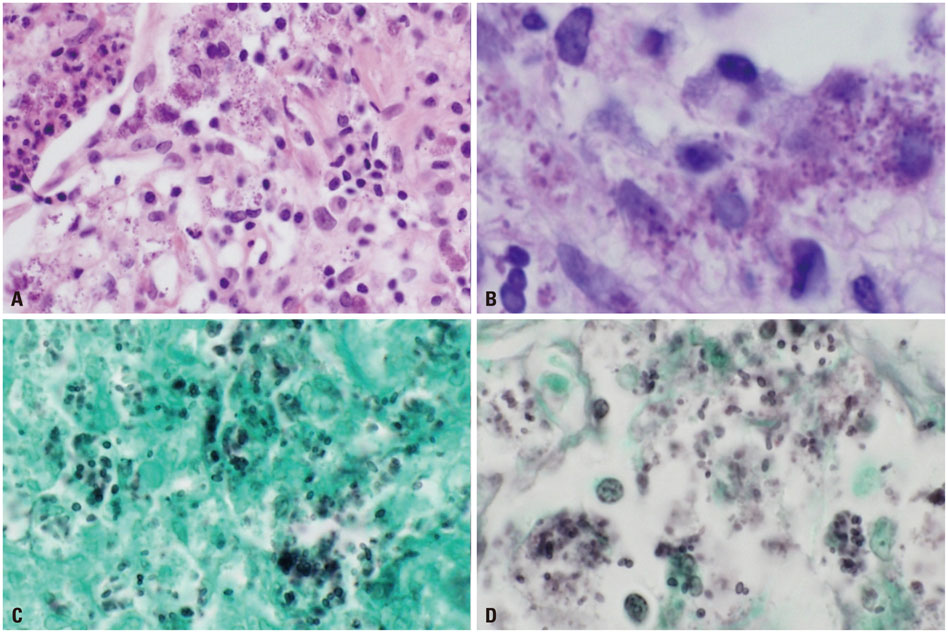
Fig. 3 Histopathologic examination of the lung. (A) Hematoxylin and eosin stain (×400). (B) Periodic acid-Schiff stain (×1000). (C) Gomori Methenamine Silver (GMS) stain (×1000). (D) Many budding yeast-form fungal microorganisms are observed in the cytoplasm of alveolar macrophages, which are clearly identified by the GMS stain (×1000).
Cited by 1 articles
-
Pulmonary Histoplasmosis Identified by Video-Assisted Thoracic Surgery (VATS) Biopsy: a Case Report
Ye Jin Lee, Hye-Rin Kang, Jin Hwa Song, Sooim Sin, Sang-Min Lee
J Korean Med Sci. 2018;33(2):. doi: 10.3346/jkms.2018.33.e15.
Reference
-
1. Wheat LJ, Freifeld AG, Kleiman MB, Baddley JW, McKinsey DS, Loyd JE, et al. Clinical practice guidelines for the management of patients with histoplasmosis: 2007 update by the Infectious Diseases Society of America. Clin Infect Dis. 2007; 45:807–825.
Article2. Wheat LJ. Histoplasmosis: a review for clinicians from non-endemic areas. Mycoses. 2006; 49:274–282.
Article3. Jeon DS, Kim JR, Chun HJ, Hong YA, Kim WT. A case of histoplasmosis diagnosed on peripheral blood smear. Korean J Hematol. 1991; 26:391–396.4. Kim HS, Kim KA, Kwon KS, Cho HG, Kim PS, Lee DH, et al. A case of histoplasma peritonitis. Inha Med J. 1999; 6:135–141.5. Jeong HW, Sohn JW, Kim MJ, Choi JW, Kim CH, Choi SH, et al. Disseminated histoplasmosis and tuberculosis in a patient with HIV infection. Yonsei Med J. 2007; 48:531–534.
Article6. McKinsey DS, McKinsey JP. Pulmonary histoplasmosis. Semin Respir Crit Care Med. 2011; 32:735–744.
Article7. Goodwin RA, Loyd JE, Des Prez RM. Histoplasmosis in normal hosts. Medicine (Baltimore). 1981; 60:231–266.
Article8. Sénéchal A, Ferry T, Boibieux A, Brion JP, Epaulard O, Chidiac C, et al. Imported pulmonary histoplasmosis in three French cavers after a trip to Cuba. J Travel Med. 2012; 19:64–65.
Article9. Dismukes WE, Royal SA, Tynes BS. Disseminated histoplasmosis in corticosteroid-treated patients. Report of five cases. JAMA. 1978; 240:1495–1498.
Article10. Lan N, Patil DT, Shen B. Histoplasma capsulatum infection in refractory Crohn's disease of the pouch on anti-TNF biological therapy. Am J Gastroenterol. 2013; 108:281–283.
Article11. Bourré-Tessier J, Fortin C, Belisle A, Desmarais E, Choquette D, Senécal JL. Disseminated Histoplasma capsulatum infection presenting with panniculitis and focal myositis in rheumatoid arthritis treated with etanercept. Scand J Rheumatol. 2009; 38:311–316.12. Hage CA, Bowyer S, Tarvin SE, Helper D, Kleiman MB, Wheat LJ. Recognition, diagnosis, and treatment of histoplasmosis complicating tumor necrosis factor blocker therapy. Clin Infect Dis. 2010; 50:85–92.
Article13. Tseng TC, Liaw SJ, Hsiao CH, Wang CY, Lee LN, Huang TS, et al. Molecular evidence of recurrent histoplasmosis with 9-year latency in a patient with Addison's disease. J Clin Microbiol. 2005; 43:4911–4913.
Article14. Murray PJ, Sladden RA. Disseminated histoplasmosis following long-term steroid therapy for reticulosarcoma. Br Med J. 1965; 2:631–632.
Article15. Kosseifi SG, Nassour DN, Shaikh MA, Sarubbi FA, Jordan RM, Peiris AN. Nodular pulmonary histoplasmosis in Cushing's disease: a case report and literature review. Tenn Med. 2007; 100:44–46.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Pulmonary Histoplasmosis Identified by Video-Assisted Thoracic Surgery (VATS) Biopsy: a Case Report
- Travel Medicine
- Histoplasmosis on bone marrow aspirate cytological examination associated with hemophagocytosis and pancytopenia in an AIDS patient
- A Case of Histoplasmosis Diagnosed on Peripheral Blood Smear
- The Safe Air Travel of the Elderly
