Unilateral versus Bilateral Groin Puncture for Atrial Fibrillation Ablation: Multi-Center Prospective Randomized Study
- Affiliations
-
- 1Department of Cardiology, Yonsei University Health System, Seoul, Korea. hnpak@yuhs.ac
- 2Department of Cardiology, Hallym University Kangnam Sacred Heart Hospital, Seoul, Korea.
- 3Department of Cardiology, Korea University Cardiovascular Center, Seoul, Korea.
- 4Department of Cardiology, Asan Medical Center, Ulsan University, Seoul, Korea.
- KMID: 2450191
- DOI: http://doi.org/10.3349/ymj.2019.60.4.360
Abstract
- PURPOSE
Catheter ablation for atrial fibrillation (AF) requires heavy anticoagulation and uncomfortable post-procedural hemostasis. We compared patient satisfaction with and the safety of unilateral groin (UG) puncture-single trans-septal (ST) ablation with conventional bilateral groin (BG) puncture-double trans-septal (DT) ablation in paroxysmal AF patients.
MATERIALS AND METHODS
We enrolled 222 patients with paroxysmal AF (59.4±10.7 years old) who were randomized in a 2:1 manner into UG-ST ablation (n=148) and BG-DT ablation (n=74) groups. If circumferential pulmonary vein isolation could not be achieved after three attempts of touch-up ablation in the UG-ST group, the patient was crossed over to BG-DT by performing a left groin puncture.
RESULTS
Ten patients in the UG-ST group (6.8%) required crossover to the BG-DT approach. There were no significant differences in procedure time (p=0.144) and major complications rate (p>0.999) between the UG-ST and BG-DT groups. Access site pain (p=0.014), back pain (p=0.023), and total pain (p=0.015) scores were significantly lower for the UG-ST than BG-DT group as assessed by the Visual Analog Scale. Over 20.2±8.7 months of follow up, there was no difference in AF recurrence free-survival rates between the two groups (Log rank, p=0.984).
CONCLUSION
UG-ST AF ablation is feasible and safe, and was found to significantly reduce post-procedural hemostasis-related discomfort, compared to the conventional DT approach, in patients with paroxysmal AF.
Keyword
MeSH Terms
Figure
-
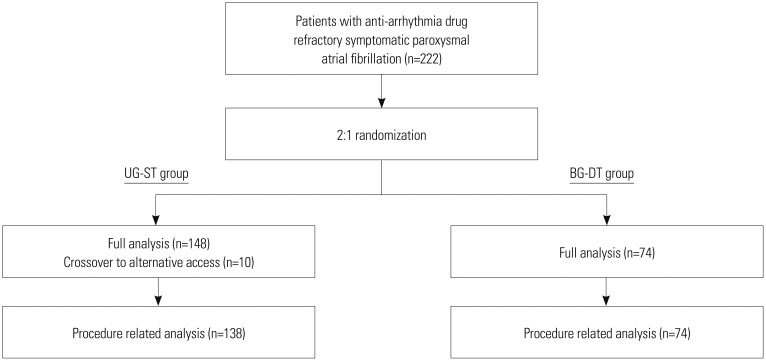
Fig. 1 Flow diagram of study population enrollment. UG-ST, unilateral groin puncture-single trans-septal; BG-DT, bilateral groin puncture-double trans-septal.
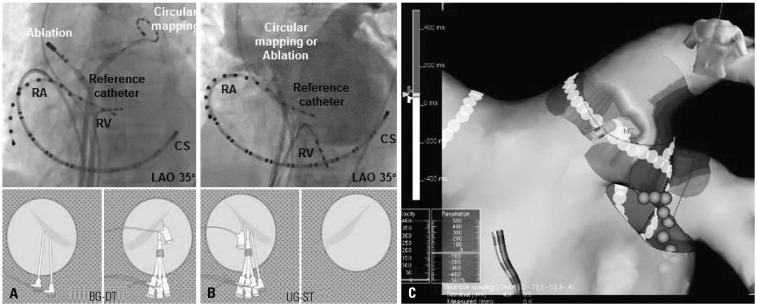
Fig. 2 Representative images of conventional bilateral groin puncture-double trans-septal ablation (BG-DT) (A) and unilateral groin puncture-single trans-septal ablation (UG-ST) (B) strategies. If there was a remnant PV potential after anatomical and local potential guided CPVI in the UG-ST group, we mapped and marked the potential PV conduction site on a three-dimensional electroanatomical map and added tough-up ablation after an additional exchange of ablation and mapping catheters (C). CPVI, circumferential pulmonary vein isolation; PV, pulmonary vein; RA, right atrium; RV, right ventricle; CS, coronary sinus; LAO, left anterior oblique.
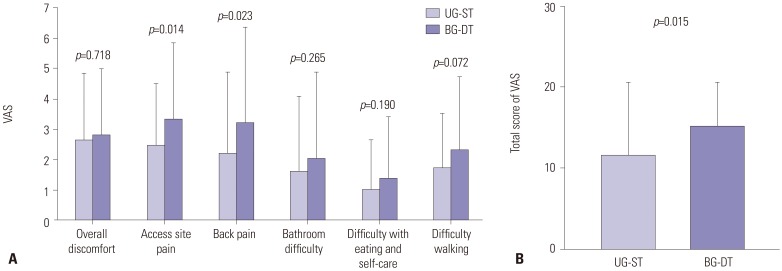
Fig. 3 Comparison of questionnaire results for post-procedural discomfort during hemostasis between the two groups. (A) Each component of quality of life was measured using a 0–10 VAS. (B) Total score of VAS results. UG-ST, unilateral groin puncture-single trans-septal; BG-DT, bilateral groin puncture-double trans-septal; VAS, visual analog scale.
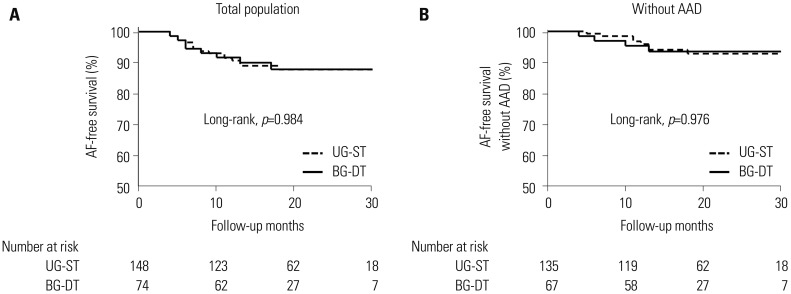
Fig. 4 Kaplan-Meier analysis of AF recurrence-free survival (A) and AF recurrence-free survival off-AAD (B) after catheter ablation between the two groups. AF, atrial fibrillation; AAD, anti-arrhythmic drug; UG-ST, unilateral groin puncture-single trans-septal; BG-DT, bilateral groin puncture-double trans-septal.
Reference
-
1. Wilber DJ, Pappone C, Neuzil P, De Paola A, Marchlinski F, Natale A, et al. Comparison of antiarrhythmic drug therapy and radiofrequency catheter ablation in patients with paroxysmal atrial fibrillation: a randomized controlled trial. JAMA. 2010; 303:333–340. PMID: 20103757.2. Kirchhof P, Benussi S, Kotecha D, Ahlsson A, Atar D, Casadei B, et al. 2016 ESC Guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur Heart J. 2016; 37:2893–2962. PMID: 27567408.
Article3. Haïssaguerre M, Jaïs P, Shah DC, Takahashi A, Hocini M, Quiniou G, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998; 339:659–666. PMID: 9725923.
Article4. Wazni OM, Marrouche NF, Martin DO, Verma A, Bhargava M, Saliba W, et al. Radiofrequency ablation vs antiarrhythmic drugs as first-line treatment of symptomatic atrial fibrillation: a randomized trial. JAMA. 2005; 293:2634–2640. PMID: 15928285.5. Haïssaguerre M, Shah DC, Jaïs P, Hocini M, Yamane T, Deisenhofer I, et al. Electrophysiological breakthroughs from the left atrium to the pulmonary veins. Circulation. 2000; 102:2463–2465. PMID: 11076817.
Article6. Oral H, Knight BP, Tada H, Ozaydin M, Chugh A, Hassan S, et al. Pulmonary vein isolation for paroxysmal and persistent atrial fibrillation. Circulation. 2002; 105:1077–1081. PMID: 11877358.
Article7. Hwang ES, Pak HN, Park SW, Park JS, Joung B, Choi D, et al. Risks and benefits of an open irrigation tip catheter in intensive radiofrequency catheter ablation in patients with non-paroxysmal atrial fibrillation. Circ J. 2010; 74:644–649. PMID: 20160395.
Article8. Shurrab M, Di Biase L, Briceno DF, Kaoutskaia A, Haj-Yahia S, Newman D, et al. Impact of contact force technology on atrial fibrillation ablation: a meta-analysis. J Am Heart Assoc. 2015; 4:e002476. PMID: 26391136.
Article9. Bertaglia E, Bella PD, Tondo C, Proclemer A, Bottoni N, De Ponti R, et al. Image integration increases efficacy of paroxysmal atrial fibrillation catheter ablation: results from the CartoMerge Italian Registry. Europace. 2009; 11:1004–1010. PMID: 19541681.10. Radulovic M, Weber C, Spiess J. The effect of acute immobilization stress on the abundance of corticotropin-releasing factor receptor in lymphoid organs. J Neuroimmunol. 2000; 103:153–164. PMID: 10696910.
Article11. Lip GY, Wang KL, Chiang CE. Non-vitamin K antagonist oral anticoagulants (NOACs) for stroke prevention in Asian patients with atrial fibrillation: time for a reappraisal. Int J Cardiol. 2015; 180:246–254. PMID: 25463377.
Article12. Kuck KH, Brugada J, Fürnkranz A, Metzner A, Ouyang F, Chun KR, et al. Cryoballoon or radiofrequency ablation for paroxysmal atrial fibrillation. N Engl J Med. 2016; 374:2235–2245. PMID: 27042964.
Article13. Shin DG, Kim TH, Uhm JS, Kim JY, Joung B, Lee MH, et al. Early experience of novel oral anticoagulants in catheter ablation for atrial fibrillation: efficacy and safety comparison to warfarin. Yonsei Med J. 2016; 57:342–349. PMID: 26847285.
Article14. Kim TH, Park J, Uhm JS, Kim JY, Joung B, Lee MH, et al. Challenging achievement of bidirectional block after linear ablation affects the rhythm outcome in patients with persistent atrial fibrillation. J Am Heart Assoc. 2016; 5:e003894. PMID: 27792644.
Article15. Kim IS, Yang PS, Kim TH, Park J, Park JK, Uhm JS, et al. Clinical significance of additional ablation of atrial premature beats after catheter ablation for atrial fibrillation. Yonsei Med J. 2016; 57:72–80. PMID: 26632385.
Article16. Cooper CJ, El-Shiekh RA, Cohen DJ, Blaesing L, Burket MW, Basu A, et al. Effect of transradial access on quality of life and cost of cardiac catheterization: a randomized comparison. Am Heart J. 1999; 138(3 Pt 1):430–436. PMID: 10467191.
Article17. Calkins H, Kuck KH, Cappato R, Brugada J, Camm AJ, Chen SA, et al. 2012 HRS/EHRA/ECAS Expert Consensus Statement on Catheter and Surgical Ablation of Atrial Fibrillation: recommendations for patient selection, procedural techniques, patient management and follow-up, definitions, endpoints, and research trial design. Europace. 2012; 14:528–606. PMID: 22389422.
Article18. Jensen MP, Chen C, Brugger AM. Interpretation of visual analog scale ratings and change scores: a reanalysis of two clinical trials of postoperative pain. J Pain. 2003; 4:407–414. PMID: 14622683.
Article19. Verma A, Jiang CY, Betts TR, Chen J, Deisenhofer I, Mantovan R, et al. Approaches to catheter ablation for persistent atrial fibrillation. N Engl J Med. 2015; 372:1812–1822. PMID: 25946280.
Article20. Cardoso R, Knijnik L, Bhonsale A, Miller J, Nasi G, Rivera M, et al. An updated meta-analysis of novel oral anticoagulants versus vitamin K antagonists for uninterrupted anticoagulation in atrial fibrillation catheter ablation. Heart Rhythm. 2018; 15:107–115. PMID: 28917562.
Article21. Aldhoon B, Wichterle D, Peichl P, Čihák R, Kautzner J. Complications of catheter ablation for atrial fibrillation in a high-volume centre with the use of intracardiac echocardiography. Europace. 2013; 15:24–32. PMID: 23015634.
Article22. Deshmukh A, Patel NJ, Pant S, Shah N, Chothani A, Mehta K, et al. In-hospital complications associated with catheter ablation of atrial fibrillation in the United States between 2000 and 2010: analysis of 93 801 procedures. Circulation. 2013; 128:2104–2112. PMID: 24061087.23. Gupta A, Perera T, Ganesan A, Sullivan T, Lau DH, Roberts-Thomson KC, et al. Complications of catheter ablation of atrial fibrillation: a systematic review. Circ Arrhythm Electrophysiol. 2013; 6:1082–1088. PMID: 24243785.
Article24. Ferguson JD, Helms A, Mangrum JM, Mahapatra S, Mason P, Bilchick K, et al. Catheter ablation of atrial fibrillation without fluoroscopy using intracardiac echocardiography and electroanatomic mapping. Circ Arrhythm Electrophysiol. 2009; 2:611–619. PMID: 20009075.
Article25. Mun HS, Joung B, Shim J, Hwang HJ, Kim JY, Lee MH, et al. Does additional linear ablation after circumferential pulmonary vein isolation improve clinical outcome in patients with paroxysmal atrial fibrillation? Prospective randomised study. Heart. 2012; 98:480–484. PMID: 22285969.
Article26. Su W, Kowal R, Kowalski M, Metzner A, Svinarich JT, Wheelan K, et al. Best practice guide for cryoballoon ablation in atrial fibrillation: the compilation experience of more than 3000 procedures. Heart Rhythm. 2015; 12:1658–1666. PMID: 25778428.
Article27. Ezzat VA, Chew A, McCready JW, Lambiase PD, Chow AW, Lowe MD, et al. Catheter ablation of atrial fibrillation-patient satisfaction from a single-center UK experience. J Interv Card Electrophysiol. 2013; 37:291–303. PMID: 23263894.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Mechanism of and Preventive Therapy for Stroke in Patients with Atrial Fibrillation
- Large Circular Ring Catheter Ablation Versus Anatomically Guided Ablation of Atrial Fibrillation: Back to the Future for Successful Catheter Ablation of Atrial Fibrillation?
- A Case of Successful Ablation of Right-Sided Accessory Pathway during Atrial Fibrillation
- Radiofrequency Catheter Ablation of Persistent Atrial Fibrillation with Myotonic Dystrophy and Achalasia-like Esophageal Dilatation
- A Totally Thoracoscopic Ablation for Persistent Atrial Fibrillation
