Efficacy and safety of cold forceps polypectomy utilizing the jumbo cup: a prospective study
- Hasegawa H

- Bamba S
- Takahashi
- Murata M
- Otsuka T
- Matsumoto
- Fujimoto T
- Osak R
- Imaeda H
- Nishida A
- Ban H
- Sonoda A
- Inatomi O
- Sasaki M
- Sugimoto M
- Andoh A
- Affiliations
-
- 1Division of Gastroenterology, Shiga University of Medical Science, Otsu, Japan.
- 2Division of Gastroenterology, Japan Community Health Care Organization Shiga Hospital, Otsu, Japan.
- 3Division of Clinical Nutrition, Shiga University of Medical Science, Otsu, Japan. sb@belle.shiga-med.ac.jp
- 4Division of Digestive Endoscopy, Shiga University of Medical Science, Otsu, Japan.
- 5Division of Gastroenterology, Kusatsu General Hospital, Kusatsu, Japan.
- KMID: 2449968
- DOI: http://doi.org/10.5217/ir.2018.00103
Abstract
- BACKGROUND/AIMS
There are few prospective studies on cold forceps polypectomy (CFP) using jumbo cup forceps. Therefore, we examined patients with diminutive polyps (5 mm or smaller) treated with CFP using jumbo cup forceps to achieve an adenoma-free colon and also assessed the safety of the procedure and the recurrence rate of missed or residual polyp after CFP by performing follow-up colonoscopy 1 year later.
METHODS
We included patients with up to 5 adenomas removed at initial colonoscopy and analyzed data from a total of 361 patients with 573 adenomas. One-year follow-up colonoscopy was performed in 165 patients, at which 251 lesions were confirmed.
RESULTS
The one-bite resection rate with CFP was highest for lesions 3 mm or smaller and decreased significantly with increasing lesion size. Post-procedural hemorrhage was observed in 1 of 573 lesions (0.17%). No perforation was noted. The definite recurrence rate was 0.8% (2/251 lesions). The probable recurrence rate, which was defined as recurrence in the same colorectal segment, was 17%. Adenoma-free colon was achieved in 55% of patients at initial resection. Multivariate analysis revealed that achievement of an adenoma-free colon was significantly associated with number of adenomas and years of endoscopic experience.
CONCLUSIONS
CFP using jumbo biopsy forceps was safe and showed a high one-bite resection rate for diminutive lesions of 3 mm or smaller. The low definite recurrence rate confirms the reliability of CFP using jumbo biopsy forceps. Number of adenomas and years of endoscopic experience were key factors in achieving an adenoma-free colon.
Keyword
MeSH Terms
Figure
-
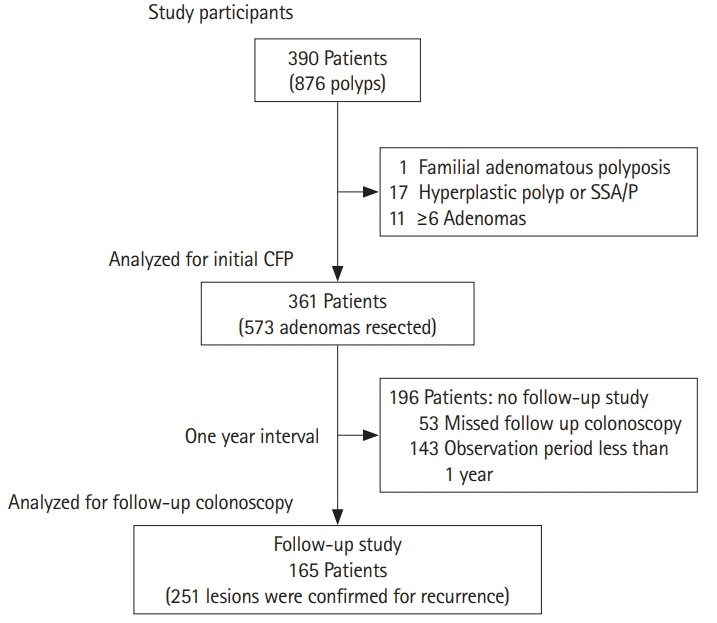
Fig. 1. Flowchart of the study participants. SSA/P, sessile serrated adenoma/polyp; CFP, cold forceps polypectomy.
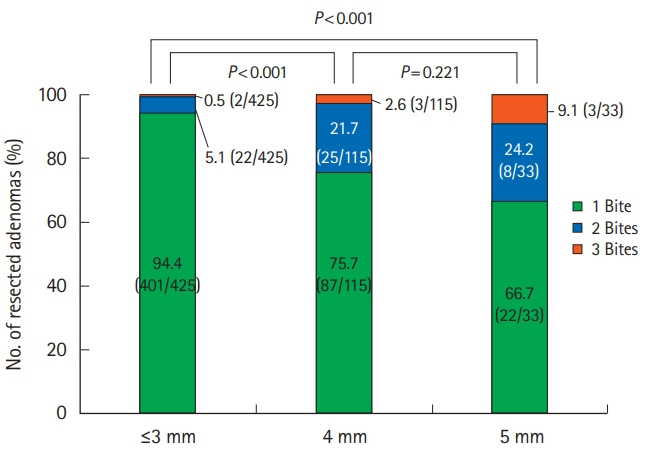
Fig. 2. One-bite resection rate and size of the adenoma. Chi-square test.
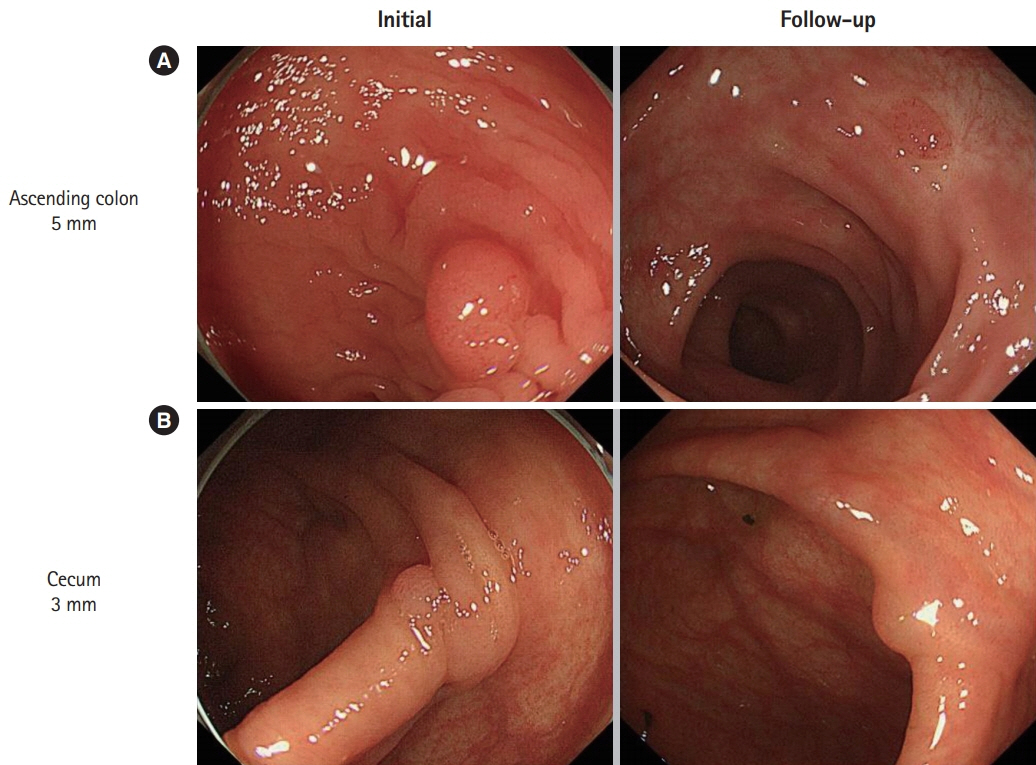
Fig. 3. Cases of definite recurrence. Recurrence of adenoma is noted in the same segment as the initial resection site. (A) Case 1: 72-year-old male, Isp polyp, 5 mm in diameter was resected with one-bite cold forceps polypectomy. The pathology was low-grade adenoma. The resection margin was diagnosed as negative. (B) Case 2: 70-year-old male, Is polyp, 3 mm in diameter was resected with one-bite cold forceps polypectomy. The pathology was low-grade adenoma. The resection margin was undetermined.
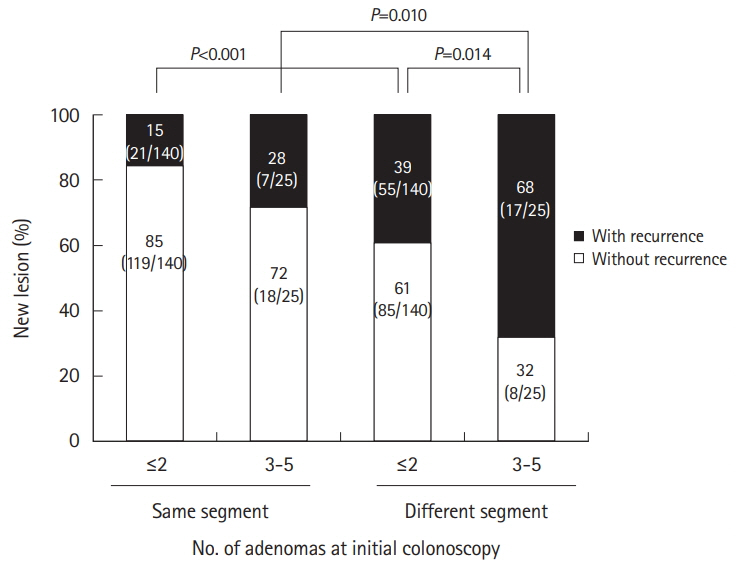
Fig. 4. Percentage of new lesions found at 1-year follow-up colonoscopy in the same segment as the original adenoma resection site at initial colonoscopy or in a different segment. Segments labeled in black represent the number of patients (with definite or probable recurrence) with a noted adenomatous lesion at the 1-year follow-up. Chi-square test.
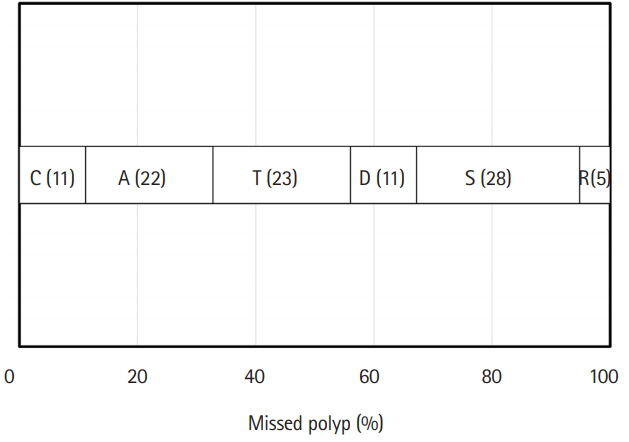
Fig. 5. Percentage of missed polyps in each segment at 1-year follow-up colonoscopy. C, cecum; A, ascending colon; T, transverse colon; D, descending colon; S, sigmoid colon; R, rectum.
Reference
-
1. Ferlay J, Soerjomataram I, Ervik M, et al. Cancer incidence and mortality worldwide. GLOBOCAN 2012 v1.0. Lyon: International Agency for Research on Cancer;2013.2. O’Keefe SJ. Diet, microorganisms and their metabolites, and colon cancer. Nat Rev Gastroenterol Hepatol. 2016; 13:691–706.
Article3. Vogelstein B, Fearon ER, Hamilton SR, et al. Genetic alterations during colorectal-tumor development. N Engl J Med. 1988; 319:525–532.
Article4. Lieberman DA, Rex DK, Winawer SJ, Giardiello FM, Johnson DA, Levin TR. Guidelines for colonoscopy surveillance after screening and polypectomy: a consensus update by the US Multi-Society Task Force on Colorectal Cancer. Gastroenterology. 2012; 143:844–857.
Article5. Atkin WS, Valori R, Kuipers EJ, et al. European guidelines for quality assurance in colorectal cancer screening and diagnosis. First edition: colonoscopic surveillance following adenoma removal. Endoscopy. 2012; 44 Suppl 3:SE151–SE163.6. Winawer SJ, Zauber AG, Ho MN, et al. Prevention of colorectal cancer by colonoscopic polypectomy: the National Polyp Study Workgroup. N Engl J Med. 1993; 329:1977–1981.
Article7. Zauber AG, Winawer SJ, O’Brien MJ, et al. Colonoscopic polypectomy and long-term prevention of colorectal-cancer deaths. N Engl J Med. 2012; 366:687–696.
Article8. Jung YS, Park JH, Kim HJ, et al. Complete biopsy resection of diminutive polyps. Endoscopy. 2013; 45:1024–1029.
Article9. Pohl H, Srivastava A, Bensen SP, et al. Incomplete polyp resection during colonoscopy-results of the complete adenoma resection (CARE) study. Gastroenterology. 2013; 144:74–80. e1.
Article10. Gómez V, Badillo RJ, Crook JE, Krishna M, Diehl NN, Wallace MB. Diminutive colorectal polyp resection comparing hot and cold snare and cold biopsy forceps polypectomy. Results of a pilot randomized, single-center study (with videos). Endosc Int Open. 2015; 3:E76–E80.
Article11. Ikematsu H, Matsuda N, Sano Y, et al. Management of polyps less than 10 mm: data from the Japan Polyp Study. Intestine. 2016; 20:457–462.12. Lee YC, Li-Sheng Chen S, Ming-Fang Yen A, et al. Association between colorectal cancer mortality and gradient fecal hemoglobin concentration in colonoscopy noncompliers. J Natl Cancer Inst. 2017; 109:djw269.
Article13. Uraoka T, Ramberan H, Matsuda T, Fujii T, Yahagi N. Cold polypectomy techniques for diminutive polyps in the colorectum. Dig Endosc. 2014; 26 Suppl 2:98–103.
Article14. Kim JS, Lee BI, Choi H, et al. Cold snare polypectomy versus cold forceps polypectomy for diminutive and small colorectal polyps: a randomized controlled trial. Gastrointest Endosc. 2015; 81:741–747.
Article15. Fujimoto K, Fujishiro M, Kato M, et al. Guidelines for gastroenterological endoscopy in patients undergoing antithrombotic treatment. Dig Endosc. 2014; 26:1–14.
Article16. Lee HS, Park HW, Lee JS, et al. Treatment outcomes and recurrence following standard cold forceps polypectomy for diminutive polyps. Surg Endosc. 2017; 31:159–169.
Article17. Endoscopic Classification Review Group. Update on the paris classification of superficial neoplastic lesions in the digestive tract. Endoscopy. 2005; 37:570–578.18. The Paris endoscopic classification of superficial neoplastic lesions: esophagus, stomach, and colon: November 30 to December 1, 2002. Gastrointest Endosc. 2003; 58(6 Suppl):S3–S43.19. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 2nd English edition. Gastric Cancer. 1998; 1:10–24.20. Sano Y, Ikematsu H, Fu KI, et al. Meshed capillary vessels by use of narrow-band imaging for differential diagnosis of small colorectal polyps. Gastrointest Endosc. 2009; 69:278–283.
Article21. Aslan F, Cekiç C, Camci M, et al. What is the most accurate method for the treatment of diminutive colonic polyps? Standard versus jumbo forceps polypectomy. Medicine (Baltimore). 2015; 94:e621.22. Draganov PV, Chang MN, Alkhasawneh A, et al. Randomized, controlled trial of standard, large-capacity versus jumbo biopsy forceps for polypectomy of small, sessile, colorectal polyps. Gastrointest Endosc. 2012; 75:118–126.
Article23. Lee CK, Shim JJ, Jang JY. Cold snare polypectomy vs. cold forceps polypectomy using double-biopsy technique for removal of diminutive colorectal polyps: a prospective randomized study. Am J Gastroenterol. 2013; 108:1593–1600.
Article24. Hirata I, Yasumoto S, Nishikawa T, Toshina K. Optimal follow-up program after colonoscopic removal of colorectal neoplasia. J Jpn Soc Coloproctol. 2006; 59:880–884.
Article25. Rex DK, Cutler CS, Lemmel GT, et al. Colonoscopic miss rates of adenomas determined by back-to-back colonoscopies. Gastroenterology. 1997; 112:24–28.
Article26. Aranda-Hernández J, Hwang J, Kandel G. Seeing better: evidence based recommendations on optimizing colonoscopy adenoma detection rate. World J Gastroenterol. 2016; 22:1767–1778.
Article27. Barclay RL, Vicari JJ, Doughty AS, Johanson JF, Greenlaw RL. Colonoscopic withdrawal times and adenoma detection during screening colonoscopy. N Engl J Med. 2006; 355:2533–2541.
Article28. Castaneda D, Popov VB, Verheyen E, Wander P, Gross SA. New technologies improve adenoma detection rate, adenoma miss rate, and polyp detection rate: a systematic review and metaanalysis. Gastrointest Endosc. 2018; 88:209–222. e11.
Article29. Clark BT, Protiva P, Nagar A, et al. Quantification of adequate bowel preparation for screening or surveillance colonoscopy in men. Gastroenterology. 2016; 150:396–405.
Article30. Kang HY, Kim D, Kim HJ, et al. The relationship between colonoscopy procedure order and adenoma detection rates: a prospective study. J Clin Gastroenterol. 2015; 49:683–689.
Article31. Maratt JK, Dickens J, Schoenfeld PS, et al. Factors associated with surveillance adenoma and sessile serrated polyp detection rates. Dig Dis Sci. 2017; 62:3579–3585.
Article32. Qayed E, Vora R, Levy S, Bostick RM. Colonoscopy procedural volume increases adenoma and polyp detection rates in gastroenterologytrainees. World J Gastrointest Endosc. 2017; 9:540–551.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Histological comparison of colon polyps by endoscopic forceps biopsy compared to polypectomy
- The Comparison of Pathologic Findings of Colonic Polyps between Forceps Biopsy and Polypectomy
- Comparative Study of Peripheral Rim Fixation Using Jumbo Cup in Revisional Hip Arthroplasty
- Endoscopic Management of Post-Polypectomy Bleeding
- Endoscopic Instruments and Electrosurgical Unit for Colonoscopic Polypectomy
