Prognostic Impact of Extended Lymph Node Dissection versus Limited Lymph Node Dissection on pN0 Proximal Advanced Gastric Cancer: a Propensity Score Matching Analysis
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. tison@yuhs.ac
- 2Gastric Cancer Center, Yonsei Cancer Center, Seoul, Korea.
- 3Department of Surgery, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- KMID: 2449942
- DOI: http://doi.org/10.5230/jgc.2019.19.e20
Abstract
- PURPOSE
Splenic hilar lymph node dissection (LND) during total gastrectomy is regarded as the standard treatment for proximal advanced gastric cancer (AGC). This study aimed to investigate whether splenic hilar LND or D2 LND is essential for proximal AGC of pT2-4aN0M0 stage.
MATERIALS AND METHODS
Data of curative total gastrectomies (n=370) performed from 2000 to 2010 for proximal AGC of pT2-4aN0 stage were retrospectively reviewed. Clinicopathological characteristics and long-term outcomes were compared using propensity score matching between patients who underwent splenectomy (n=43) and those who did not (n=327) and between patients who underwent D2 LND (n=122) and those who underwent D1+ LND (n=248).
RESULTS
Tumors of larger size and a more advanced T stage and significantly lower overall and relapse-free survival (P<0.001) were observed in the splenectomy group than in the 2 spleen-preserving groups. Before propensity score matching, worse overall and relapse-free survival (P<0.001) was observed in the splenectomy group than in the non-splenectomy group. After matching, although the overall survival became similar (P=0.123), relapse-free survival was worse in the splenectomy group (P=0.021). Compared with D1+ LND, D2 LND had no positive impact on the overall (P=0.619) and relapse-free survival (P=0.112) after propensity score matching.
CONCLUSIONS
Splenic hilar LND with or without splenectomy may not have an oncological benefit for patients with pathological AGC with no LN metastasis.
Keyword
MeSH Terms
Figure
-
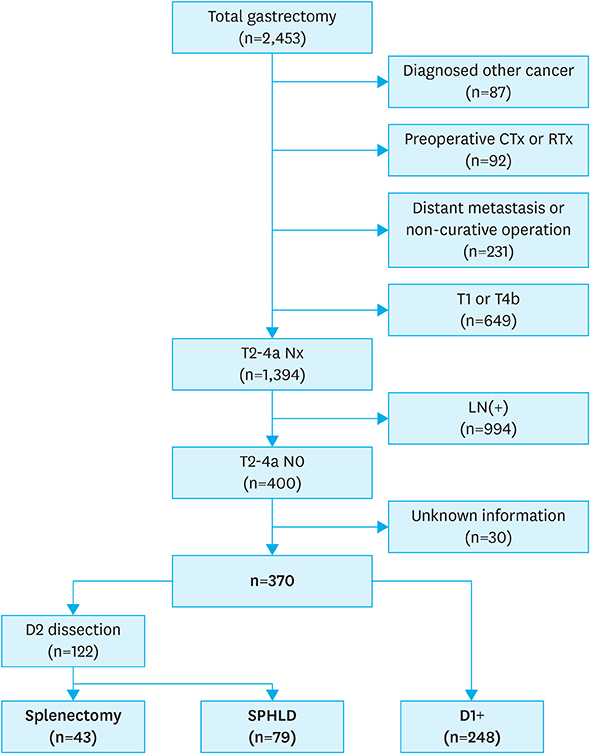
Fig. 1 Study profile.

Fig. 2 Kaplan-Meier overall and relapse-free survival curves for patients with splenectomy, SPHLD, and D1+ groups. (A) Overall survival among the 3 groups. (B) R-free survival among the 3 groups. SPHLD = spleen-preserving hilar lymph node dissection.
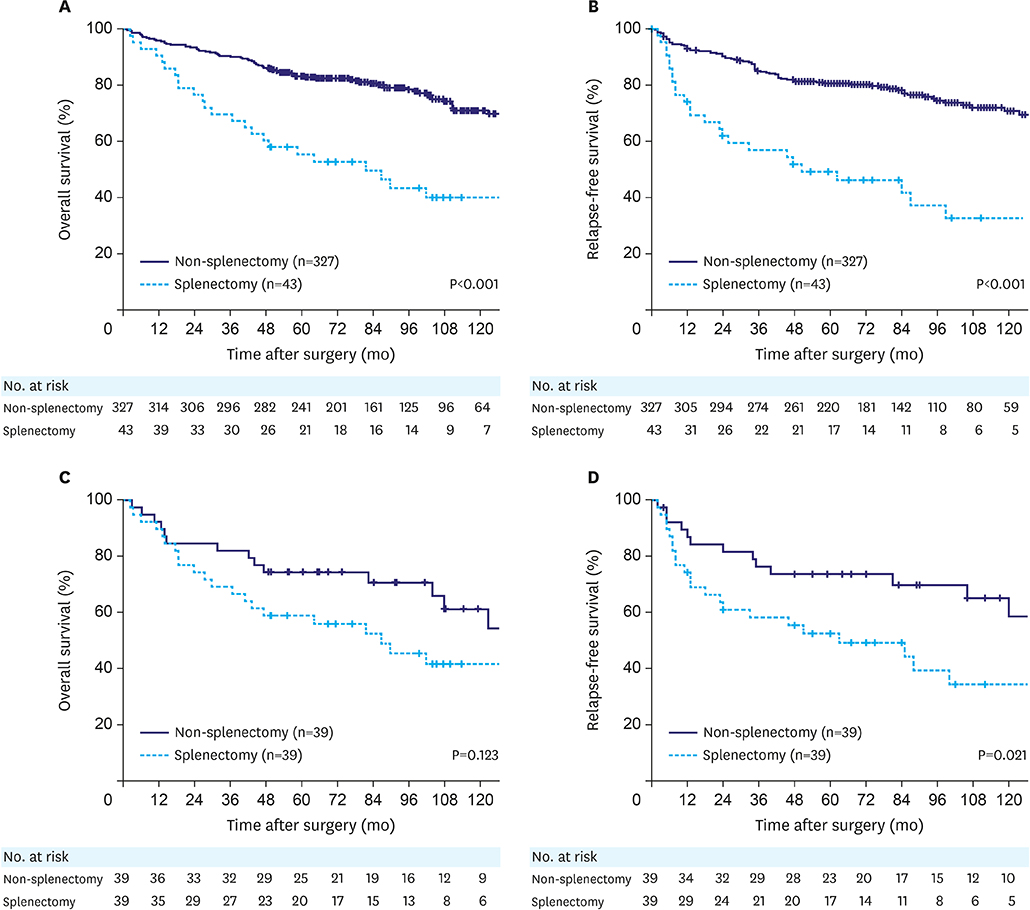
Fig. 3 Kaplan-Meier overall and relapse-free survival curves for patients with splenectomy compared with those for patients with non-splenectomy (SPHLD+D1+) before and after propensity score matching. (A) Overall survival before matching (P<0.001). (B) Relapse-free survival before matching (P<0.001). (C) Overall survival after matching (P=0.123). (D) Relapse-free survival after matching (P=0.021). SPHLD = spleen-preserving hilar lymph node dissection.

Fig. 4 Kaplan-Meier overall and relapse-free survival curves for patients with D2 LN dissection (splenectomy+SPHLD) compared with those for patients with D1+ before and after propensity score matching. (A) Overall survival before matching (P=0.001). (B) Relapse-free survival before matching (P<0.001). (C) Overall survival after matching (P=0.619). (D) Relapse-free survival after matching (P=0.112). SPHLD = spleen-preserving hilar lymph node dissection.
Reference
-
1. Songun I, Putter H, Kranenbarg EM, Sasako M, van de Velde CJ. Surgical treatment of gastric cancer: 15-year follow-up results of the randomised nationwide Dutch D1D2 trial. Lancet Oncol. 2010; 11:439–449.
Article2. Sano T, Sasako M, Yamamoto S, Nashimoto A, Kurita A, Hiratsuka M, et al. Gastric cancer surgery: morbidity and mortality results from a prospective randomized controlled trial comparing D2 and extended para-aortic lymphadenectomy--Japan Clinical Oncology Group study 9501. J Clin Oncol. 2004; 22:2767–2773.
Article3. Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer. 2015; 136:E359–E386.
Article4. Blot WJ, Devesa SS, Kneller RW, Fraumeni JF Jr. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991; 265:1287–1289.
Article5. Ikeguchi M, Kaibara N. Lymph node metastasis at the splenic hilum in proximal gastric cancer. Am Surg. 2004; 70:645–648.6. Meyer HJ, Jähne J, Weimann A, Pichlmayr R. Surgical therapy of stomach cancer--indications for splenectomy in gastrectomy. Chirurg. 1994; 65:437–440.7. Mönig SP, Collet PH, Baldus SE, Schmackpfeffer K, Schröder W, Thiele J, et al. Splenectomy in proximal gastric cancer: frequency of lymph node metastasis to the splenic hilus. J Surg Oncol. 2001; 76:89–92.8. Yu W, Choi GS, Chung HY. Randomized clinical trial of splenectomy versus splenic preservation in patients with proximal gastric cancer. Br J Surg. 2006; 93:559–563.
Article9. Japanese Gastric Cancer Association. Japanese classification of gastric carcinoma: 3rd English edition. Gastric Cancer. 2011; 14:101–112.10. Maruyama K, Okabayashi K, Kinoshita T. Progress in gastric cancer surgery in Japan and its limits of radicality. World J Surg. 1987; 11:418–425.
Article11. Kosuga T, Ichikawa D, Okamoto K, Komatsu S, Shiozaki A, Fujiwara H, et al. Survival benefits from splenic hilar lymph node dissection by splenectomy in gastric cancer patients: relative comparison of the benefits in subgroups of patients. Gastric Cancer. 2011; 14:172–177.
Article12. Bonenkamp JJ, Hermans J, Sasako M, van de Velde CJ, Welvaart K, Songun I, et al. Extended lymph-node dissection for gastric cancer. N Engl J Med. 1999; 340:908–914.
Article13. Cuschieri A, Weeden S, Fielding J, Bancewicz J, Craven J, Joypaul V, et al. Patient survival after D1 and D2 resections for gastric cancer: long-term results of the MRC randomized surgical trial. Br J Cancer. 1999; 79:1522–1530.
Article14. Hyung WJ, Lim JS, Song J, Choi SH, Noh SH. Laparoscopic spleen-preserving splenic hilar lymph node dissection during total gastrectomy for gastric cancer. J Am Coll Surg. 2008; 207:e6–e11.
Article15. Oh SJ, Hyung WJ, Li C, Song J, Kang W, Rha SY, et al. The effect of spleen-preserving lymphadenectomy on surgical outcomes of locally advanced proximal gastric cancer. J Surg Oncol. 2009; 99:275–280.
Article16. Maehara Y, Moriguchi S, Yoshida M, Takahashi I, Korenaga D, Sugimachi K. Splenectomy does not correlate with length of survival in patients undergoing curative total gastrectomy for gastric carcinoma. Univariate and multivariate analyses. Cancer. 1991; 67:3006–3009.
Article17. Sano T, Sasako M, Mizusawa J, Yamamoto S, Katai H, Yoshikawa T, et al. Randomized controlled trial to evaluate splenectomy in total gastrectomy for proximal gastric carcinoma. Ann Surg. 2017; 265:277–283.
Article18. Sano T, Yamamoto S, Sasako M. Japan Clinical Oncology Group Study LCOG 0110-MF. Randomized controlled trial to evaluate splenectomy in total gastrectomy for proximal gastric carcinoma: Japan clinical oncology group study JCOG 0110-MF. Jpn J Clin Oncol. 2002; 32:363–364.
Article19. Son T, Kwon IG, Lee JH, Choi YY, Kim HI, Cheong JH, et al. Impact of splenic hilar lymph node metastasis on prognosis in patients with advanced gastric cancer. Oncotarget. 2017; 8:84515–84528.
Article20. Watanabe M, Kinoshita T, Enomoto N, Shibasaki H, Nishida T. Clinical significance of splenic hilar dissection with splenectomy in advanced proximal gastric cancer: an analysis at a single institution in Japan. World J Surg. 2016; 40:1165–1171.
Article21. Ji X, Fu T, Bu ZD, Zhang J, Wu XJ, Zong XL, et al. Comparison of different methods of splenic hilar lymph node dissection for advanced upper- and/or middle-third gastric cancer. BMC Cancer. 2016; 16:765.
Article22. Kinoshita T. Splenic hilar dissection in the treatment of proximal advanced gastric cancer: what is an adequate strategy? Transl Gastroenterol Hepatol. 2016; 1:72.
Article23. Tsendsuren T, Jun SM, Mian XH. Usefulness of endoscopic ultrasonography in preoperative TNM staging of gastric cancer. World J Gastroenterol. 2006; 12:43–47.
Article24. Tokunaga M, Ito S, Yoshikawa T, Nunobe S, Fukagawa T, Misawa K, et al. Prognostic factors for survival in patients with pT1 N+ or T2–3 N0 gastric cancer in Japan. Br J Surg. 2017; 104:885–890.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advantages of Splenic Hilar Lymph Node Dissection in Proximal Gastric Cancer Surgery
- A Clinical Analysis of the Characteristics of the Lymph Node Metastasis in Patients with Gastrics Cancer
- Disadvantages of Complete No. 10 Lymph Node Dissection in Gastric Cancer and the Possibility of Spleen-Preserving Dissection: Review
- Prognostic Significance of the Extent of Lymph Node Dissection in Gastric Cancer
- Treatment of Malignant Melanoma Using Sentinel Lymph Node Dissection
