Is it Possible to Successfully Treat Locally Advanced Colon Cancer Using Pre-Operative Chemoradiotherapy?
- Affiliations
-
- 1Department of Internal Medicine, Kosin University College of Medicine, Busan, Korea. parksj6406@hanmail.net
- 2Department of Colorectal Surgery, Kosin University College of Medicine, Busan, Korea.
- 3Department of Radiology, Kosin University College of Medicine, Busan, Korea.
- KMID: 2447678
- DOI: http://doi.org/10.5946/ce.2018.088
Abstract
- Pre-operative chemoradiotherapy (CRT) is a preferable treatment option for patients with locally advanced rectal cancer. However, few data are available regarding pre-operative CRT for locally advanced colon cancer. Here, we describe two cases of successful treatment with pre-operative CRT and establish evidence supporting this treatment option in patients with locally advanced colon cancer. In the first case, a 65-year-old woman was diagnosed with ascending colon cancer with duodenal invasion. In the second case, a 63-year-old man was diagnosed with a colonic-duodenal fistula due to transverse colon cancer invasion. These case reports will help to establish a treatment consensus for pre-operative CRT in patients with locally advanced colon cancer.
Keyword
MeSH Terms
Figure
-
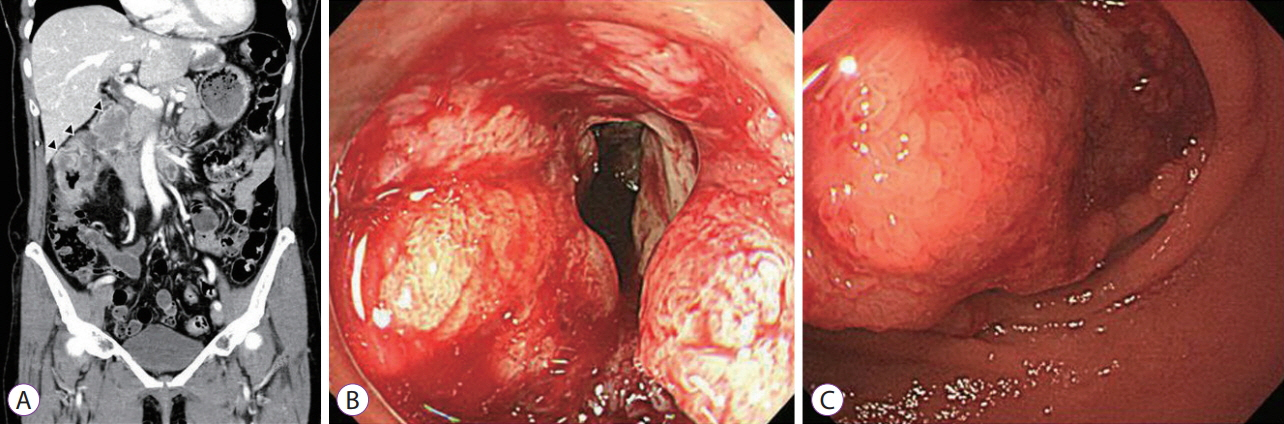
Fig. 1. (A) Abdominal computed tomography revealed fat stranding around the ascending colon with irregular wall thickening and a 1.5-cm, low-density lesion on the duodeno-pancreatic groove (black arrowhead). (B) Colonoscopic examination showed an ulcero-infiltrative mass with luminal narrowing. (C) Upper endoscopic examination showed a large exophytic mass with obstruction in the second portion of the duodenum.
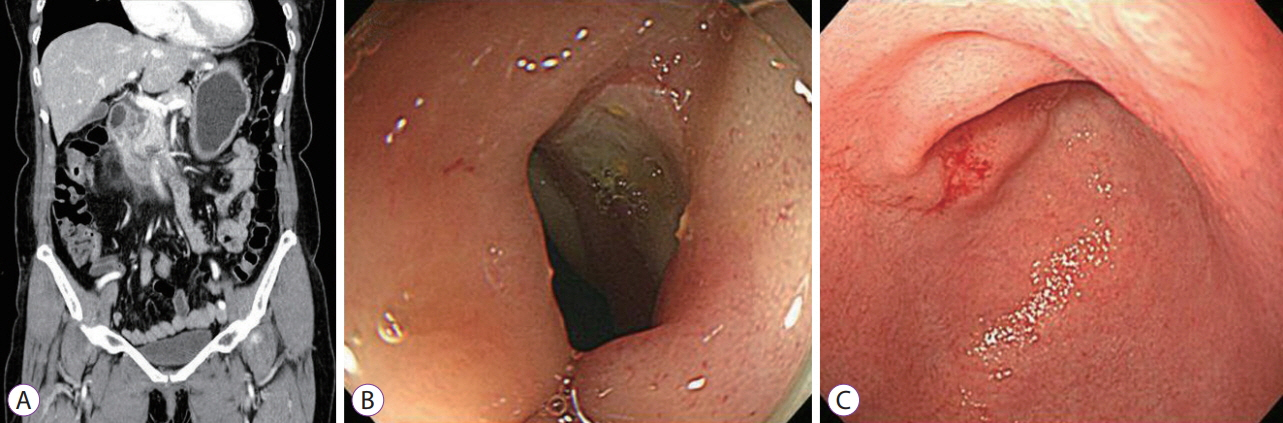
Fig. 2. (A) Abdominal computed tomography revealed reduced irregularly enhancing wall thickening at the ascending colon. (B, C) Colonoscopic and upper endoscopic examination revealed significantly reduced tumors compared to previous studies.
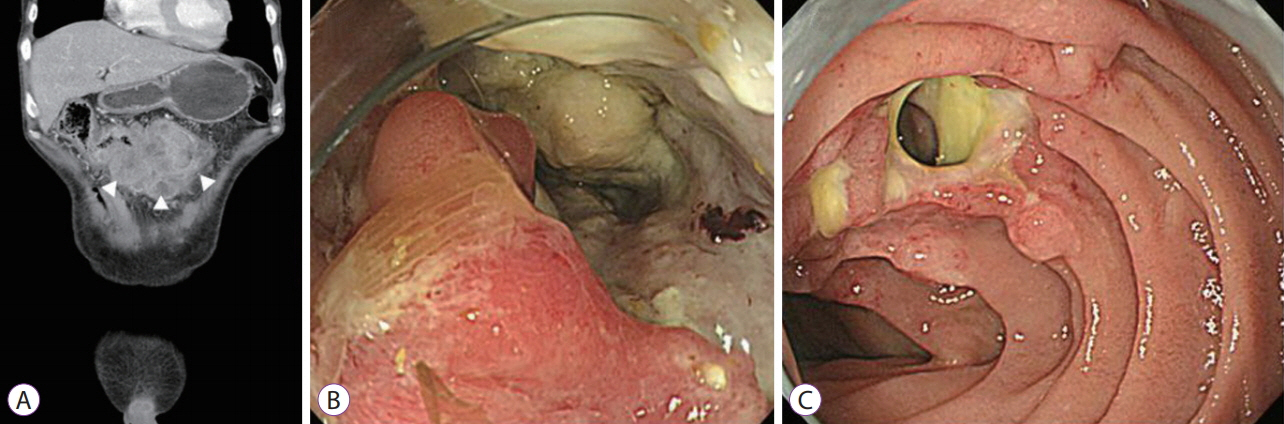
Fig. 3. (A) Computed tomography image showing a large irregular mass at the transverse colon extending to and invading the duodenum. (B) Colonoscopic images showed poorly circumscribed infiltrating masses with ulceration in the transverse colon. (C) Upper endoscopic examination showed a 2-cm fistula tract covered with yellowish exudates.
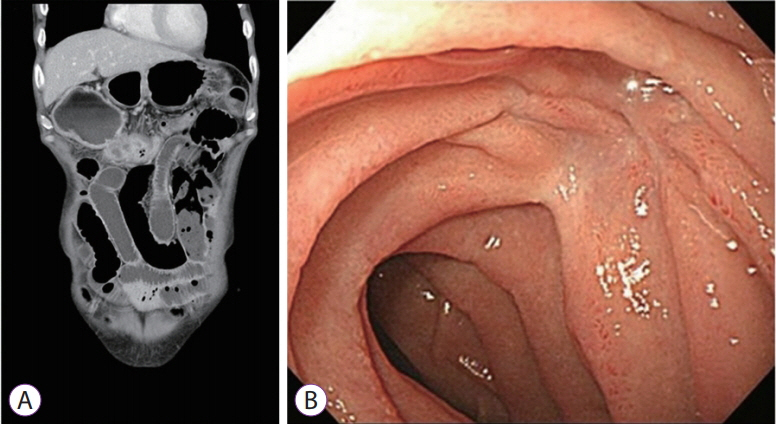
Fig. 4. Abdominal computed tomography revealed decreased size of the enhancing lobulated mass in the transverse colon and alleviated invasion of the adjacent anterior abdominal wall and duodenum (A). Upper endoscopic examination showed that the fistula opening was closed and replaced with a white scar (B).
Reference
-
1. Bevan R, Rutter MD. Colorectal cancer screening-who, how, and when? Clin Endosc. 2018; 51:37–49.
Article2. Govindarajan A, Fraser N, Cranford V, et al. Predictors of multivisceral resection in patients with locally advanced colorectal cancer. Ann Surg Oncol. 2008; 15:1923–1930.
Article3. Staniunas RJ, Schoetz DJ Jr. Extended resection for carcinoma of colon and rectum. Surg Clin North Am. 1993; 73:117–129.
Article4. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: rectal cancer version 3. 2017 [Internet]. Fort Washington (PA): National Comprehensive Cancer Network;c2017. [cited 2017 Mar 13]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/rectal.pdf.5. Sauer R, Becker H, Hohenberger W, et al. Preoperative versus postoperative chemoradiotherapy for rectal cancer. N Engl J Med. 2004; 351:1731–1740.
Article6. National Comprehensive Cancer Network. NCCN clinical practice guidelines in oncology: colon cancer version 2. 2017 [Internet]. Fort Washington (PA): National Comprehensive Cancer Network;c2017. [cited 2017 Mar 13]. Available from: https://www.nccn.org/professionals/physician_gls/pdf/colon.pdf.7. Sauer R, Liersch T, Merkel S, et al. Preoperative versus postoperative chemoradiotherapy for locally advanced rectal cancer: results of the German CAO/ARO/AIO-94 randomized phase III trial after a median follow-up of 11 years. J Clin Oncol. 2012; 30:1926–1933.
Article8. Khrizman P, Niland JC, ter Veer A, et al. Postoperative adjuvant chemotherapy use in patients with stage II/III rectal cancer treated with neoadjuvant therapy: a national comprehensive cancer network analysis. J Clin Oncol. 2013; 31:30–38.
Article9. Franke AJ, Parekh H, Starr JS, Tan SA, Iqbal A, George TJ Jr. Total neoadjuvant therapy: a shifting paradigm in locally advanced rectal cancer management. Clin Colorectal Cancer. 2018; 17:1–12.
Article10. Kalyan A, Rozelle S, Benson A 3rd. Neoadjuvant treatment of rectal cancer: where are we now? Gastroenterol Rep (Oxf). 2016; 4:206–209.
Article11. Agranovich A, Berthelet E. Radiotherapy for colorectal cancer. B C Med J. 2000; 42:139–141.12. Curley SA, Carlson GW, Shumate CR, Wishnow KI, Ames FC. Extended resection for locally advanced colorectal carcinoma. Am J Surg. 1992; 163:553–559.
Article13. Curley SA, Evans DB, Ames FC. Resection for cure of carcinoma of the colon directly invading the duodenum or pancreatic head. J Am Coll Surg. 1994; 179:587–592.14. Taylor WE, Donohue JH, Gunderson LL, et al. The Mayo Clinic experience with multimodality treatment of locally advanced or recurrent colon cancer. Ann Surg Oncol. 2002; 9:177–185.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Long Term Complete Response of Unresectable Locally Advanced Pancreatic Cancer after CCRT and Gemcitabine Chemotherapy
- Preoperative Concurrent Chemoradiotherapy with Oral Fluoropyrimidine in Locally Advanced Rectal Cancer: How Good Is Good Enough?
- Does the Addition of Adjuvant Chemotherapy to Concurrent Chemoradiotherapy Improve the Survival of Patients with Locally Advanced Nasopharyngeal Cancer?
- Surgical issues in locally advanced rectal cancer treated by preoperative chemoradiotherapy
- The Effects and Surgical Morbidity of Preoperative Combined Chemoradiotherapy for Locally Advanced Rectal Cancer
