Subtrochanteric Fracture Reduction during Intramedullary Nailing: Technical Note
- Affiliations
-
- 1Department of Orthopedic Surgery, Inje University Haeundae Paik Hospital, Busan, Korea. docos@naver.com
- KMID: 2443113
- DOI: http://doi.org/10.12671/jkfs.2019.32.2.107
Abstract
- The subtrochanteric area is the place where mechanical stress is most concentrated in the femur. When a fracture happens, bone union is delayed and nonunion often occurs. The recommended treatment for atypical fractures is an anatomical reduction of the fracture site as the frequency of nonunion is higher than that of ordinary fractures. Various reduction methods have been suggested, and good results have been obtained. On the other hand, the occurrence of posterior displacement of the distal fragment during the insertion of an intramedullary nail is often overlooked. This is probably because the bone marrow of the femur tends to form an elliptical shape in the anteroposterior direction. The author attempted to insert a blocking screw into the distal part of the fracture to prevent posterior displacement of the distal fragment while performing intramedullary nailing of the femur fracture and achieved a good reduction state easily.
Figure
-
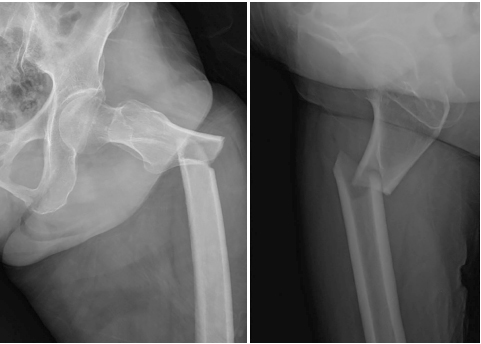
Fig. 1 Initial radiographs of a 76-year-old woman showing an atypical fracture of the subtrochanteric region of the femur.

Fig. 2 Internal fixation was performed with a long-length proximal femoral nail antirotation, and a single poller screw was inserted into the anterior part of the intramedullary nail. A distal locking screw was inserted in dynamic mode (arrows).

Fig. 3 Complete bone union was achieved 5 months after surgery.
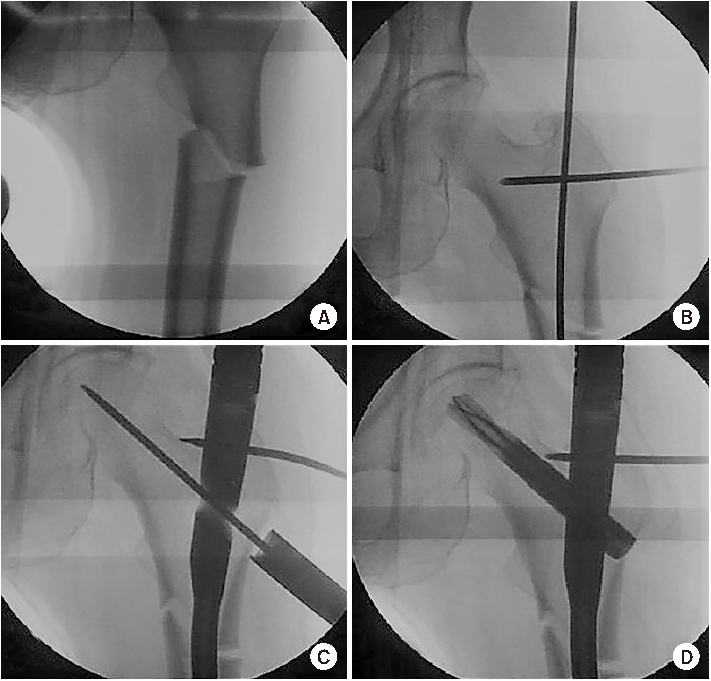
Fig. 4 (A, B) External rotation and abduction deformity of the proximal fragment was corrected by inserting the Steinmann pin for the joy stick method, which was followed by advancing a straight guide wire through the proper entry point. (C, D) In the anteroposterior view, the reduction of the fracture appeared to be good.
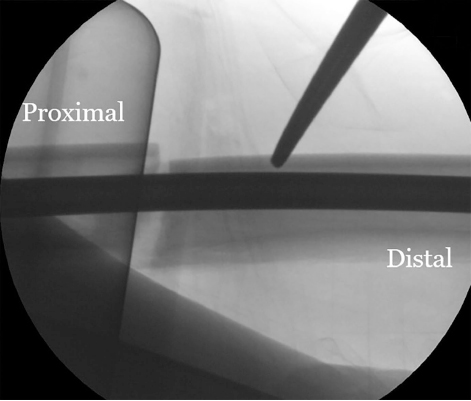
Fig. 5 When the marrow canal is wide, the distal fragment is displaced posteriorly.

Fig. 6 (A) With traction of the leg and maintaining the fracture gap, insert a Steinmann pin through the lateral side cortical bone and make contact with the front of the intramedullary nail while entering. (B, C) With the far cortical bone not passing through, if lifting the pin out of the skin, the distal bone fragment moves forward and the posterior displacement is corrected. (D) After obtaining anatomical alignment, if the traction released, the gap of the fracture part decreases, and appropriate reduction can be achieved.
Reference
-
1. Kuzyk PR, Bhandari M, McKee MD, Russell TA, Schemitsch EH. Intramedullary versus extramedullary fixation for subtrochanteric femur fractures. J Orthop Trauma. 2009; 23:465–470.
Article2. Park SH, Kong GM, Ha BH, Park JH, Kim KH. Nonunion of subtrochanteric fractures: comminution or malreduction. Pak J Med Sci. 2016; 32:591–594.
Article3. An KC, Park DH, Kong GM, Kim JY, Kim SB, Sakong SY. Treatment and prognosis of femoral insufficiency fracture associated with prolonged bisphosphonate use. J Korean Fract Soc. 2014; 27:10–16.
Article4. Kweon SH, Yoo BM. Radiologic and serologic factors associated with bone union at femoral atypical fracture. J Korean Fract Soc. 2019; 32:27–34.
Article5. Yang KH. Correction of malalignment during subtrochanteric nailing. J Korean Fract Soc. 2009; 22:66–70.
Article6. Pape HC, Tarkin IS. Intraoperative reduction techniques for difficult femoral fractures. J Orthop Trauma. 2009; 23:S6–S11.
Article7. Pak CH, Lee SH, Ha SH, Lee GC, Song KC. The treatment of subtrochanteric fractures with proximal femoral nail antirotation. J Korean Fract Soc. 2013; 26:284–291.
Article8. Saini P, Kumar R, Shekhawat V, Joshi N, Bansal M, Kumar S. Biological fixation of comminuted subtrochanteric fractures with proximal femur locking compression plate. Injury. 2013; 44:226–231.
Article9. Lim HS, Kim CK, Park YS, Moon YW, Lim SJ, Kim SM. Factors associated with increased healing time in complete femoral fractures after long-term bisphosphonate therapy. J Bone Joint Surg Am. 2016; 98:1978–1987.
Article10. Stedtfeld HW, Mittlmeier T, Landgraf P, Ewert A. The logic and clinical applications of blocking screws. J Bone Joint Surg Am. 2004; 86:Suppl 2. 17–25.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Subtrochanteric Fracture: Emphasis on Surgical Techniques in Nailing
- Efficacy of Percutaneous Cerclage Wiring in Intramedullary Nailing of Subtrochanteric Femur Fracture: Technical Note
- Interlocking Intramedullary Nailing Versus conventional Kuntscher Intramedullary Nailing for Fracture of the Femoral Shaft
- Extraction of Misplaced Endcap during Tibia Intramedullary Nailing by 'Fish-Hook' Technique: Technical Note
- Fracture of Femur Neck Associated with Technical Errors in Closed Intramedullary Nailing of the Femur
