Quantitative Thoracic Magnetic Resonance Criteria for the Differentiation of Cysts from Solid Masses in the Anterior Mediastinum
- Affiliations
-
- 1Department of Radiology, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea. yshoka@gmail.com
- 2Siemens Healthineers, Seoul, Korea.
- 3Department of Radiology, Seoul National University Bundang Hospital, Seongnam, Korea.
- 4Department of Radiology and Center for Imaging Science, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 5Department of Radiology, Massachusetts General Hospital, Harvard Medical School, Boston, MA, USA.
- KMID: 2442719
- DOI: http://doi.org/10.3348/kjr.2018.0699
Abstract
OBJECTIVE
To evaluate quantitative magnetic resonance imaging (MRI) parameters for differentiation of cysts from and solid masses in the anterior mediastinum.
MATERIALS AND METHODS
The development dataset included 18 patients from two institutions with pathologically-proven cysts (n = 6) and solid masses (n = 12) in the anterior mediastinum. We measured the maximum diameter, normalized T1 and T2 signal intensity (nT1 and nT2), normalized apparent diffusion coefficient (nADC), and relative enhancement ratio (RER) of each lesion. RERs were obtained by non-rigid registration and subtraction of precontrast and postcontrast T1-weighted images. Differentiation criteria between cysts and solid masses were identified based on receiver operating characteristics analysis. For validation, two separate datasets were utilized: 15 patients with 8 cysts and 7 solid masses from another institution (validation dataset 1); and 11 patients with clinically diagnosed cysts stable for more than two years (validation dataset 2). Sensitivity and specificity were calculated from the validation datasets.
RESULTS
nT2, nADC, and RER significantly differed between cysts and solid masses (p = 0.032, 0.013, and < 0.001, respectively). The following criteria differentiated cysts from solid masses: RER < 26.1%; nADC > 0.63; nT2 > 0.39. In validation dataset 1, the sensitivity of the RER, nADC, and nT2 criteria was 87.5%, 100%, and 75.0%, and the specificity was 100%, 40.0%, and 57.4%, respectively. In validation dataset 2, the sensitivity of the RER, nADC, and nT2 criteria was 90.9%, 90.9%, and 72.7%, respectively.
CONCLUSION
Quantitative MRI criteria using nT2, nADC, and particularly RER can assist differentiation of cysts from solid masses in the anterior mediastinum.
Keyword
MeSH Terms
Figure
-
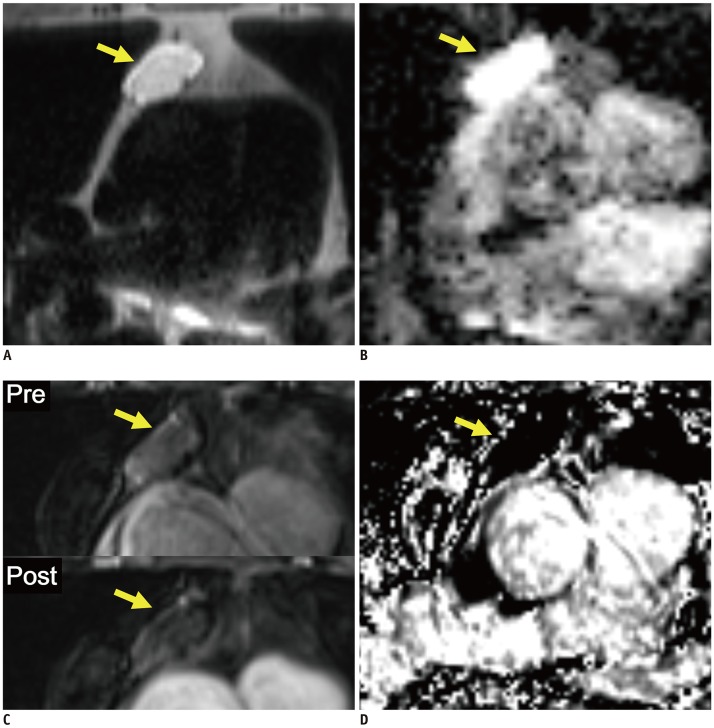
Fig. 1 Representative case from development dataset (cyst).Axial T2-weighted HASTE image (A), ADC map (B), pre- and post-contrast fat-suppressed T1-weighted images (C), and RER map (D) from 70-year-old male patient revealed 3.1 cm mass in anterior mediastinum (arrows). nT2, nADC, and RER values were 0.92, 1.50, and 5.3%, respectively. Pathologic diagnosis after surgical resection was thymic cyst. ADC = apparent diffusion coefficient, HASTE = half-Fourier-acquired single-shot turbo spin echo, nADC = normalized ADC, nT2 = normalized T2 signal intensity, RER = relative enhancement ratio
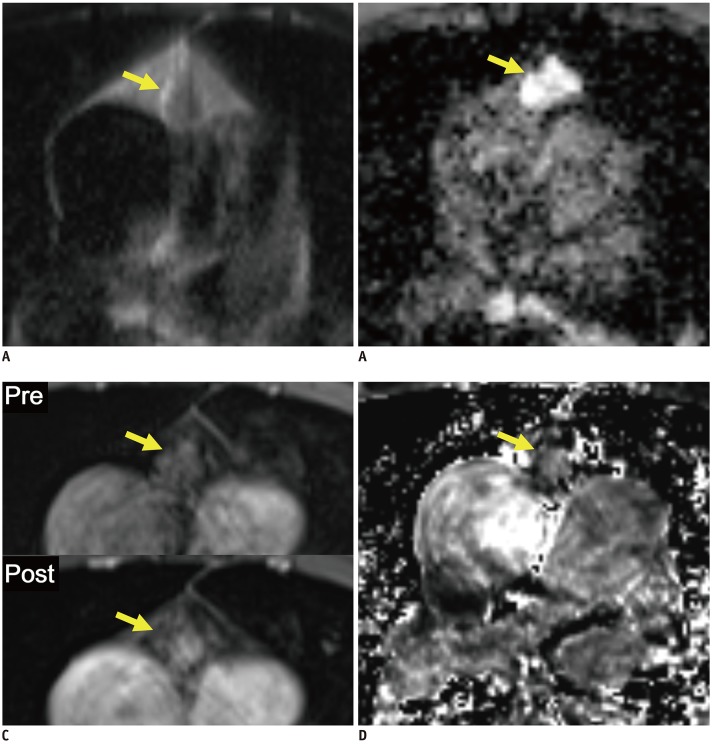
Fig. 2 Representative case from development dataset (solid mass).Axial T2-weighted HASTE image (A), ADC map (B), pre- and post-contrast fat-suppressed T1-weighted images (C), and RER map (D) from 65-year-old male patient revealed 1.6 cm mass in anterior mediastinum (arrows). nT2, nADC, and RER values were 0.32, 0.76, and 59.6%, respectively. Pathologic diagnosis after surgical resection was thymoma, type B2.
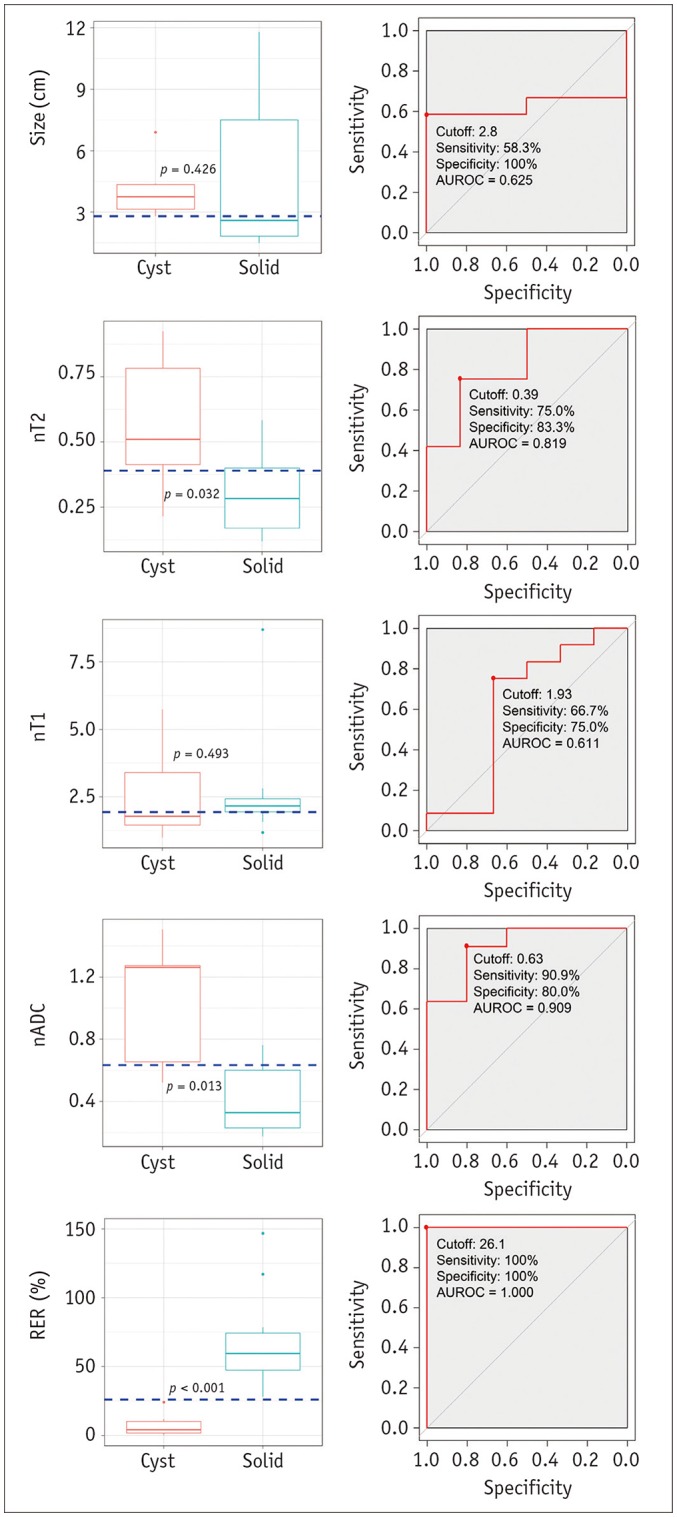
Fig. 3 Boxplots and ROC curves for differentiation between cysts and solid masses in development dataset.Boxplots in left column show results of comparison of image variables between cysts and solid masses. nT2, nADC, and RER differed significantly between cysts and solid masses. Horizontal dashed lines indicate cutoff values developed in ROC analyses. ROC curves in right column show results of ROC analyses for differentiation between cysts and solid masses. Although nT2, and nADC appeared to be significant variables, RER showed perfect separation between cysts and solid masses. nT2, nT1, and nADC are fraction values without units. AUROC = area under receiver operating characteristic curve, ROC = receiver operating characteristic
Cited by 1 articles
-
Significant Abnormalities Other than Lung Cancer in Korean Lung Cancer CT Screening
Soon Ho Yoon, Junghee Hong, Eui Jin Hwang, Heekyung Kim, Hyun-ju Lim, Young Joo Suh, Hyae Young Kim, Jin Mo Goo
J Korean Soc Radiol. 2019;80(5):837-848. doi: 10.3348/jksr.2019.80.5.837.
Reference
-
1. Araki T, Nishino M, Gao W, Dupuis J, Washko GR, Hunninghake GM, et al. Anterior mediastinal masses in the framingham heart study: prevalence and CT image characteristics. Eur J Radiol Open. 2015; 2:26–31. PMID: 25705709.
Article2. Henschke CI, Lee IJ, Wu N, Farooqi A, Khan A, Yankelevitz D, et al. CT screening for lung cancer: prevalence and incidence of mediastinal masses. Radiology. 2006; 239:586–590. PMID: 16641357.3. Yoon SH, Choi SH, Kang CH, Goo JM. Incidental anterior mediastinal nodular lesions on chest CT in asymptomatic subjects. J Thorac Oncol. 2018; 13:359–366. PMID: 29233791.4. Shahrzad M, Le TS, Silva M, Bankier AA, Eisenberg RL. Anterior mediastinal masses. AJR Am J Roentgenol. 2014; 203:W128–W138. PMID: 25055288.
Article5. Ackman JB, Verzosa S, Kovach AE, Louissaint A Jr, Lanuti M, Wright CD, et al. High rate of unnecessary thymectomy and its cause. Can computed tomography distinguish thymoma, lymphoma, thymic hyperplasia, and thymic cysts? Eur J Radiol. 2015; 84:524–533. PMID: 25575742.
Article6. Carter BW, Okumura M, Detterbeck FC, Marom EM. Approaching the patient with an anterior mediastinal mass: a guide for radiologists. J Thorac Oncol. 2014; 9(9 Suppl 2):S110–S118. PMID: 25396307.
Article7. Tomiyama N, Honda O, Tsubamoto M, Inoue A, Sumikawa H, Kuriyama K, et al. Anterior mediastinal tumors: diagnostic accuracy of CT and MRI. Eur J Radiol. 2009; 69:280–288. PMID: 18023547.
Article8. Birnbaum BA, Hindman N, Lee J, Babb JS. Renal cyst pseudoenhancement: influence of multidetector CT reconstruction algorithm and scanner type in phantom model. Radiology. 2007; 244:767–775. PMID: 17709828.
Article9. Jurado J, Javidfar J, Newmark A, Lavelle M, Bacchetta M, Gorenstein L, et al. Minimally invasive thymectomy and open thymectomy: outcome analysis of 263 patients. Ann Thorac Surg. 2012; 94:974–981. discussion 981-982. PMID: 22748641.
Article10. Kent MS, Wang T, Gangadharan SP, Whyte RI. What is the prevalence of a “nontherapeutic” thymectomy? Ann Thorac Surg. 2014; 97:276–282. discussion 282. PMID: 24140214.
Article11. Ackman JB, Gaissert HA, Lanuti M, Digumarthy SR, Shepard JA, Halpern EF, et al. Impact of nonvascular thoracic MR imaging on the clinical decision making of thoracic surgeons: a 2-year prospective study. Radiology. 2016; 280:464–474. PMID: 26909650.
Article12. Ackman JB, Wu CC. MRI of the thymus. AJR Am J Roentgenol. 2011; 197:W15–W20. PMID: 21700977.
Article13. Merine DS, Fishman EK, Zerhouni EA. Computed tomography and magnetic resonance imaging diagnosis of thymic cyst. J Comput Tomogr. 1988; 12:220–222. PMID: 3168543.
Article14. Inaoka T, Takahashi K, Mineta M, Yamada T, Shuke N, Okizaki A, et al. Thymic hyperplasia and thymus gland tumors: differentiation with chemical shift MR imaging. Radiology. 2007; 243:869–876. PMID: 17463136.15. Zhang W, Zhou Y, Xu XQ, Kong LY, Xu H, Yu TF, et al. A whole-tumor histogram analysis of apparent diffusion coefficient maps for differentiating thymic carcinoma from lymphoma. Korean J Radiol. 2018; 19:358–365. PMID: 29520195.
Article16. Ackman JB. MR imaging of mediastinal masses. Magn Reson Imaging Clin N Am. 2015; 23:141–164. PMID: 25952512.
Article17. Carter BW, Betancourt SL, Benveniste MF. MR imaging of mediastinal masses. Top Magn Reson Imaging. 2017; 26:153–165. PMID: 28777164.
Article18. Shin KE, Yi CA, Kim TS, Lee HY, Choi YS, Kim HK, et al. Diffusion-weighted MRI for distinguishing non-neoplastic cysts from solid masses in the mediastinum: problem-solving in mediastinal masses of indeterminate internal characteristics on CT. Eur Radiol. 2014; 24:677–684. PMID: 24177751.
Article19. Bae KT, Heiken JP, Siegel CL, Bennett HF. Renal cysts: is attenuation artifactually increased on contrast-enhanced CT images? Radiology. 2000; 216:792–796. PMID: 10966713.
Article20. Maki DD, Birnbaum BA, Chakraborty DP, Jacobs JE, Carvalho BM, Herman GT. Renal cyst pseudoenhancement: beam-hardening effects on CT numbers. Radiology. 1999; 213:468–472. PMID: 10551228.
Article21. Ho VB, Allen SF, Hood MN, Choyke PL. Renal masses: quantitative assessment of enhancement with dynamic MR imaging. Radiology. 2002; 224:695–700. PMID: 12202701.
Article22. Romeo V, Esposito A, Maurea S, Camera L, Mainenti PP, Palmieri G, et al. Correlative imaging in a patient with cystic thymoma: CT, MR and PET/CT comparison. Pol J Radiol. 2015; 80:22–26. PMID: 25593635.
Article23. Daye D, Ackman JB. Characterization of mediastinal masses by MRI: techniques and applications. Appl Radiol. 2017; 46:10–22.
