Transcanal Endoscopic Ear Surgery for Congenital Cholesteatoma
- Affiliations
-
- 1Department of Otorhinolaryngology-Head and Neck Surgery, Dongguk University Ilsan Hospital, Goyang, Korea.
- 2Department of Otorhinolaryngology-Head and Neck Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. moonij@skku.edu
- KMID: 2439849
- DOI: http://doi.org/10.21053/ceo.2018.00122
Abstract
OBJECTIVES
As endoscopic instrumentation, techniques and knowledges have significantly improved recently, endoscopic ear surgery has become increasingly popular. Transcanal endoscopic ear surgery (TEES) can provide better visualization of hidden areas in the middle ear cavity during congenital cholesteatoma removal. We aimed to describe outcomes for TEES for congenital cholesteatoma in a pediatric population.
METHODS
Twenty-five children (age, 17 months to 9 years) with congenital cholesteatoma confined to the middle ear underwent TEES by an experienced surgeon; 13 children had been classified as Potsic stage I, seven as stage II, and five as stage III. The mean follow-up period was 24 months. Recurrence of congenital cholesteatoma and surgical complication was observed.
RESULTS
Congenital cholesteatoma can be removed successfully via transcanal endoscopic approach in all patients, and no surgical complications occurred; only one patient with a stage II cholesteatoma showed recurrence during the follow-up visit, and the patient underwent revision surgery. The other patients underwent one-stage operations and showed no cholesteatoma recurrence at their last visits. Two patients underwent second-stage ossicular reconstruction.
CONCLUSION
Although the follow-up period and number of patients were limited, pediatric congenital cholesteatoma limited to the middle ear cavity could be safely and effectively removed using TEES.
MeSH Terms
Figure
-
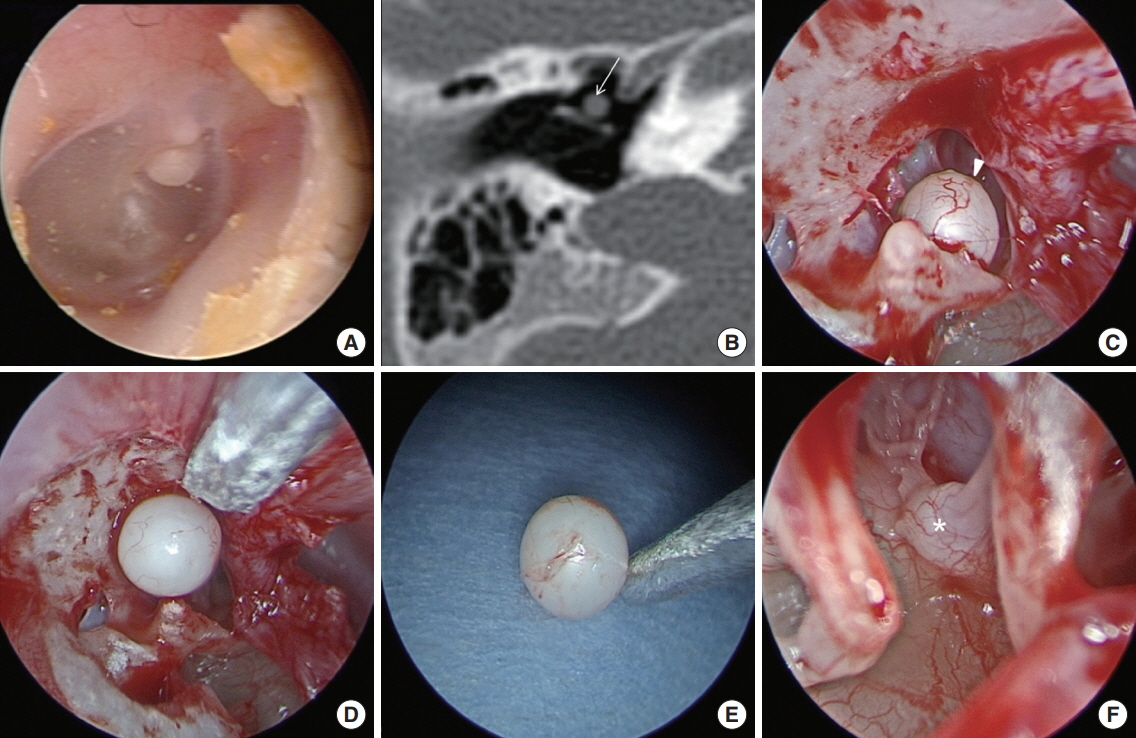
Fig. 1. Preoperative and operative findings in case 18. (A) Endoscopic findings revealed a white round mass behind the anterior superior quadrant of the tympanic membrane. (B) Computed tomography showed a well-defined round mass of soft tissue density at the anterior aspect of the malleus handle (arrow). A closed-type cholesteatoma (arrowhead) was recognized after a tympanomeatal flap was elevated (C) and removed completely (D, E). (F) The absence of congenital cholesteatoma was confirmed in the tympanic cavity including the cochleariform process (asterisk).

Fig. 2. Preoperative findings in case 13. (A) Endoscopic findings revealed a white round mass behind the inferior half of the intact tympanic membrane. (B) Pure tone audiometry revealed conductive hearing loss of 25 dB air-bone gap in the right ear (red lines), while left hearing was normal (blue line). (C, D) Preoperative computed tomography scans demonstrated a mass of soft tissue density occupying the mesotympanum and extending sinus tympani with ossicular destruction.

Fig. 3. Operative findings in case 13. (A) Endoscopic findings revealed a large white mass occupying the tympanum behind the tympanomeatal flap. (B) The cholesteatoma was too large to remove en bloc, so it was opened and reduced in size by removing inner keratin debris. The cholesteatoma was carefully dissected from the surrounding structure while the surgeon was careful not to lose hold of the sac (arrow). The anterior part of the cholesteatoma was carefully dissected from the surrounding structure (C) and completely removed including in the posterior tympanum (arrows; D, E). (F) The absence of congenital cholesteatoma (CC) was confirmed in the tympanic cavity. CT, chorda tympani; Mh, malleus handle; S, stapes; RW, round window niche.

Fig. 4. Postoperative findings in case 13. An endoscopic exam (A) and computed tomography scans (B, C, axial and coronal) showed no residual or recurrent cholesteatoma at 10-month follow-up. Air-bone gap in the right ear (red lines; left ear, blue line) (D) after the first operation, in which the destructed incus was removed with the congenital cholesteatoma, decreased substantially (E) after the second stage ossiculoplasty performed 1 year after congenital cholesteatoma removal.
Cited by 1 articles
-
Endoscopic Ear Surgery: Paradigm Shift or Subordinate Role?
Il Joon Moon, Sung Huhn Kim
Clin Exp Otorhinolaryngol. 2019;12(2):103-104. doi: 10.21053/ceo.2019.00220.
Reference
-
1. McGill TJ, Merchant S, Healy GB, Friedman EM. Congenital cholesteatoma of the middle ear in children: a clinical and histopathological report. Laryngoscope. 1991; Jun. 101(6 Pt 1):606–13.2. Lim HW, Yoon TH, Kang WS. Congenital cholesteatoma: clinical features and growth patterns. Am J Otolaryngol. 2012; Sep-Oct. 33(5):538–42.
Article3. James AL. Endoscopic middle ear surgery in children. Otolaryngol Clin North Am. 2013; Apr. 46(2):233–44.
Article4. Marchioni D, Soloperto D, Rubini A, Villari D, Genovese E, Artioli F, et al. Endoscopic exclusive transcanal approach to the tympanic cavity cholesteatoma in pediatric patients: our experience. Int J Pediatr Otorhinolaryngol. 2015; Mar. 79(3):316–22.
Article5. Potsic WP, Samadi DS, Marsh RR, Wetmore RF. A staging system for congenital cholesteatoma. Arch Otolaryngol Head Neck Surg. 2002; Sep. 128(9):1009–12.
Article6. Friedberg J. Congenital cholesteatoma. Laryngoscope. 1994; Mar. 104(3 Pt 2):1–24.
Article7. Doyle KJ, Luxford WM. Congenital aural cholesteatoma: results of surgery in 60 cases. Laryngoscope. 1995; Mar. 105(3 Pt 1):263–7.
Article8. Chen JM, Schloss MD, Manoukian JJ, Shapiro RS. Congenital cholesteatoma of the middle ear in children. J Otolaryngol. 1989; Feb. 18(1):44–8.9. Sanna M, Zini C, Bacciu S. Surgery for cholesteatoma in children. In : Tos M, Thomsen J, Peitersen E, editors. Cholesteatoma and mastoid surgery. Amsterdam: Kugler and Ghedini Publication;1989. p. 685–8.10. Migirov L, Shapira Y, Horowitz Z, Wolf M. Exclusive endoscopic ear surgery for acquired cholesteatoma: preliminary results. Otol Neurotol. 2011; Apr. 32(3):433–6.11. Kakehata S, Futai K, Sasaki A, Shinkawa H. Endoscopic transtympanic tympanoplasty in the treatment of conductive hearing loss: early results. Otol Neurotol. 2006; Jan. 27(1):14–9.
Article12. Tarabichi M. Endoscopic management of acquired cholesteatoma. Am J Otol. 1997; Sep. 18(5):544–9.13. Kobayashi T, Gyo K, Komori M, Hyodo M. Efficacy and safety of transcanal endoscopic ear surgery for congenital cholesteatomas: a preliminary report. Otol Neurotol. 2015; Dec. 36(10):1644–50.14. Kozin ED, Gulati S, Kaplan AB, Lehmann AE, Remenschneider AK, Landegger LD, et al. Systematic review of outcomes following observational and operative endoscopic middle ear surgery. Laryngoscope. 2015; May. 125(5):1205–14.
Article15. James AL, Cushing S, Papsin BC. Residual cholesteatoma after endoscope-guided surgery in children. Otol Neurotol. 2016; Feb. 37(2):196–201.
Article16. Hunter JB, Zuniga MG, Sweeney AD, Bertrand NM, Wanna GB, Haynes DS, et al. Pediatric endoscopic cholesteatoma surgery. Otolaryngol Head Neck Surg. 2016; Jun. 154(6):1121–7.
Article17. Ghadersohi S, Carter JM, Hoff SR. Endoscopic transcanal approach to the middle ear for management of pediatric cholesteatoma. Laryngoscope. 2017; Nov. 127(11):2653–8.
Article18. Hanna BM, Kivekas I, Wu YH, Guo LJ, Lin H, Guidi J, et al. Minimally invasive functional approach for cholesteatoma surgery. Laryngoscope. 2014; Oct. 124(10):2386–92.
Article19. Levenson MJ, Parisier SC, Chute P, Wenig S, Juarbe C. A review of twenty congenital cholesteatomas of the middle ear in children. Otolaryngol Head Neck Surg. 1986; Jun. 94(5):560–7.
Article20. Kojima H, Tanaka Y, Shiwa M, Sakurai Y, Moriyama H. Congenital cholesteatoma clinical features and surgical results. Am J Otolaryngol. 2006; Sep-Oct. 27(5):299–305.
Article21. Hidaka H, Yamaguchi T, Miyazaki H, Nomura K, Kobayashi T. Congenital cholesteatoma is predominantly found in the posterior-superior quadrant in the Asian population: systematic review and meta-analysis, including our clinical experience. Otol Neurotol. 2013; Jun. 34(4):630–8.22. Kim YH, Yoo JC, Lee JH, Oh SH, Chang SO, Koo JW, et al. Stage progression of congenital cholesteatoma in children. Eur Arch Otorhinolaryngol. 2012; Mar. 269(3):833–7.
Article23. Darrouzet V, Duclos JY, Portmann D, Bebear JP. Congenital middle ear cholesteatomas in children: our experience in 34 cases. Otolaryngol Head Neck Surg. 2002; Jan. 126(1):34–40.
Article24. Inokuchi G, Okuno T, Hata Y, Baba M, Sugiyama D. Congenital cholesteatoma: posterior lesions and the staging system. Ann Otol Rhinol Laryngol. 2010; Jul. 119(7):490–4.
Article25. Stapleton AL, Egloff AM, Yellon RF. Congenital cholesteatoma: predictors for residual disease and hearing outcomes. Arch Otolaryngol Head Neck Surg. 2012; Mar. 138(3):280–5.26. Yamatodani T, Mizuta K, Hosokawa K, Takizawa Y, Sugiyama K, Nakanishi H, et al. Congenital middle ear cholesteatoma: experience from 26 surgical cases. Ann Otol Rhinol Laryngol. 2013; May. 122(5):316–21.
Article27. Marchioni D, Alicandri-Ciufelli M, Molteni G, Villari D, Monzani D, Presutti L. Ossicular chain preservation after exclusive endoscopic transcanal tympanoplasty: preliminary experience. Otol Neurotol. 2011; Jun. 32(4):626–31.28. Tarabichi M. Endoscopic management of limited attic cholesteatoma. Laryngoscope. 2004; Jul. 114(7):1157–62.
Article29. Marchioni D, Alicandri-Ciufelli M, Piccinini A, Genovese E, Monzani D, Tarabichi M, et al. Surgical anatomy of transcanal endoscopic approach to the tympanic facial nerve. Laryngoscope. 2011; Jul. 121(7):1565–73.
Article30. Thomassin JM, Korchia D, Doris JM. Endoscopic-guided otosurgery in the prevention of residual cholesteatomas. Laryngoscope. 1993; Aug. 103(8):939–43.
Article31. Ito T, Kubota T, Watanabe T, Futai K, Furukawa T, Kakehata S. Transcanal endoscopic ear surgery for pediatric population with a narrow external auditory canal. Int J Pediatr Otorhinolaryngol. 2015; Dec. 79(12):2265–9.
Article32. Cohen MS, Landegger LD, Kozin ED, Lee DJ. Pediatric endoscopic ear surgery in clinical practice: lessons learned and early outcomes. Laryngoscope. 2016; Mar. 126(3):732–8.
Article33. Kazahaya K, Potsic WP. Congenital cholesteatoma. Curr Opin Otolaryngol Head Neck Surg. 2004; Oct. 12(5):398–403.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Intratympanic Membrane Congenital Cholesteatoma
- A Case of Two Isolated Congenital Cholesteatomas Presented in Middle Ear Cavity
- Usefulness of Endoscopic Removal of Congenital Cholesteatoma in Children
- Minimally Invasive Transcanal Removal of Attic Cholesteatoma
- A Case of Congenital Cholesteatoma : Combined with Ossicular Anomaly
