Primary malignant melanoma of the uterine cervix treated with pembrolizumab after radical surgery: a case report and literature review
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. bksong.kim@samsung.com
- 2Division of Hematology-Oncology, Department of Internal Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- KMID: 2439727
- DOI: http://doi.org/10.5468/ogs.2018.61.4.524
Abstract
- Malignant melanoma of the genital tract is a rare disease that is usually diagnosed by chance. When a definite diagnosis is delayed, the prognosis is very poor without standardized treatment. Herein, we describe a 40-year-old patient who presented with a history of bloody vaginal discharge for 7 months. Gynecological examination showed an exophytic, hard and pigmented cervical mass involving the upper vagina. The patient was diagnosed with cervical melanoma after a punch biopsy and underwent a radical hysterectomy, upper vaginectomy, bilateral salpingo-oophorectomy and pelvic lymphadenectomy. After surgeries, the patient underwent 2-cycles of adjuvant immunotherapy with pembrolizumab, but died within 8 months. In this report, treatment with pembrolizumab after radical surgery was not effective for this patient who had a primary cervical melanoma that metastasized to bone and lung tissue. We do not know why pembrolizumab was ineffective for this patient, but there are several possible explanations; further research is needed.
MeSH Terms
Figure
-
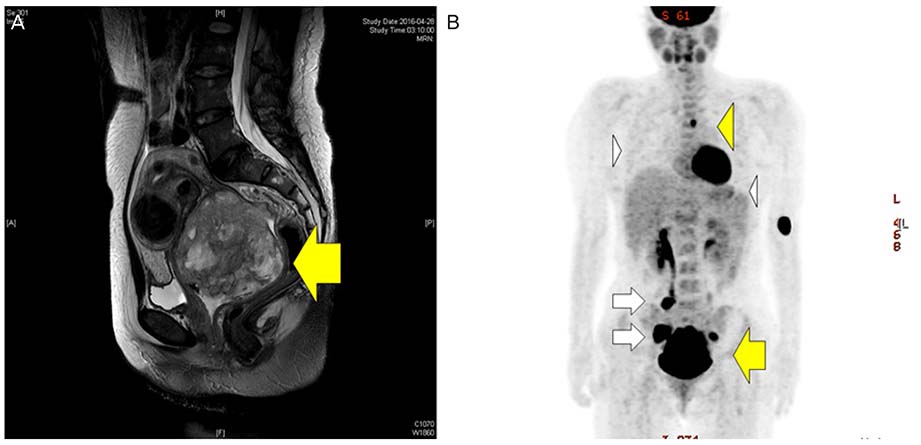
Fig. 1 (A) Pelvis magnetic resonance imaging showing melanoma of the cervix (arrow). The lesion was 9.5×7.5 cm and had invaded the upper vagina. (B) A large hypermetabolic mass with increased fluorodeoxyglucose uptake of maximum standardized uptake value (SUVmax=17.1) in the uterine cervix (large arrow). Bone metastases were observed with increased fluorodeoxyglucose uptake in T4 (SUVmax=8.6) and L5 (SUVmax=6.7) spins (large arrowhead). Right common iliac, bilateral internal iliac, and right perirectal area lymph node metastases were observed (small arrow). Small pulmonary nodules suspected because pulmonary metastases were observed in the right middle and left lower lobes of the lungs. Multiple pleural nodules suspected because pleural metastases were observed in the left lung (small arrowhead).
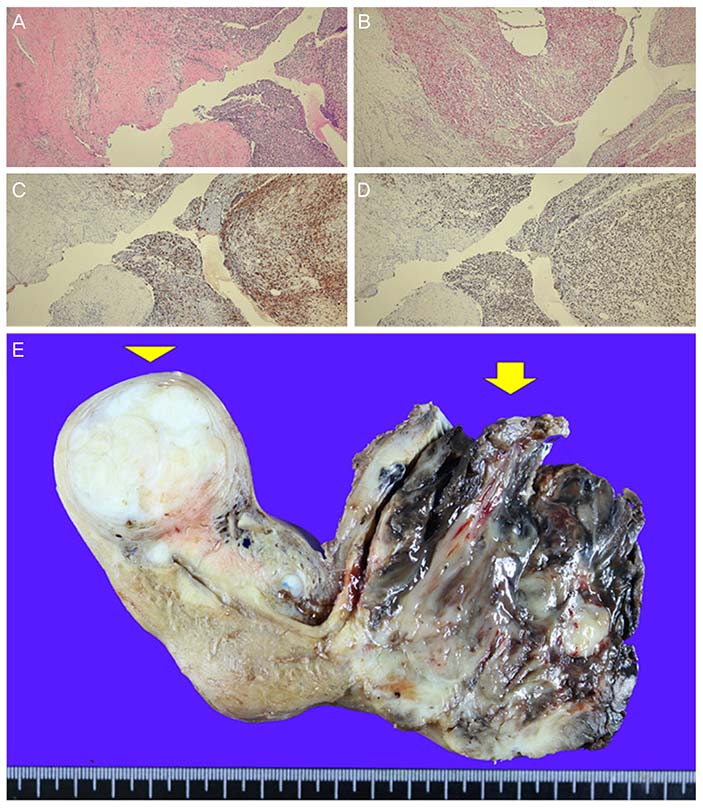
Fig. 2 (A) Infiltrative tumor cells (hematoxylin and eosin, magnification ×200). (B-D) Immunohistochemical positivity for Melan-A, HMB45, and Ki-67 (magnification ×200). (E) Gross features of the mass showing melanoma of cervix: the lesion is located in the posterior portion of the cervix, approximately 7×7 cm in size, and contains a black portion (arrow). A leiomyoma of about 4×4 cm is located in the uterine body (arrowhead).
Reference
-
1. Patrick RJ, Fenske NA, Messina JL. Primary mucosal melanoma. J Am Acad Dermatol. 2007; 56:828–834.
Article2. Myriokefalitaki E, Babbel B, Smith M, Ahmed AS. Primary malignant melanoma of uterine cervix FIGO IIa1: a case report with 40 months ongoing survival and literature review. Gynecol Oncol Case Rep. 2013; 5:52–54.3. Cid JM. Melanoid pigmentation of the endocervix: a neurogenic visceral argument. Ann Anat Pathol (Paris). 1959; 4:617–628.4. Mordel N, Mor-Yosef S, Ben-Baruch N, Anteby SO. Malignant melanoma of the uterine cervix: case report and review of the literature. Gynecol Oncol. 1989; 32:375–380.
Article5. Garbe C, Peris K, Hauschild A, Saiag P, Middleton M, Bastholt L, et al. Diagnosis and treatment of melanoma. European consensus-based interdisciplinary guideline - Update 2016. Eur J Cancer. 2016; 63:201–217.
Article6. van Zeijl MC, van den Eertwegh AJ, Haanen JB, Wouters MW. (Neo)adjuvant systemic therapy for melanoma. Eur J Surg Oncol. 2017; 43:534–543.
Article7. Colombino M, Capone M, Lissia A, Cossu A, Rubino C, De Giorgi V, et al. BRAF/NRAS mutation frequencies among primary tumors and metastases in patients with melanoma. J Clin Oncol. 2012; 30:2522–2529.
Article8. Zak KM, Kitel R, Przetocka S, Golik P, Guzik K, Musielak B, et al. Structure of the complex of human programmed death 1, PD-1, and its ligand PD-L1. Structure. 2015; 23:2341–2348.
Article9. Robert C, Ribas A, Wolchok JD, Hodi FS, Hamid O, Kefford R, et al. Anti-programmed-death-receptor-1 treatment with pembrolizumab in ipilimumab-refractory advanced melanoma: a randomised dose-comparison cohort of a phase 1 trial. Lancet. 2014; 384:1109–1117.
Article10. Ribas A, Hamid O, Daud A, Hodi FS, Wolchok JD, Kefford R, et al. Association of pembrolizumab with tumor response and survival among patients with advanced melanoma. JAMA. 2016; 315:1600–1609.
Article11. Ribas A, Puzanov I, Dummer R, Schadendorf D, Hamid O, Robert C, et al. Pembrolizumab versus investigator-choice chemotherapy for ipilimumab-refractory melanoma (KEYNOTE-002): a randomised, controlled, phase 2 trial. Lancet Oncol. 2015; 16:908–918.12. Robert C, Schachter J, Long GV, Arance A, Grob JJ, Mortier L, et al. Pembrolizumab versus ipilimumab in advanced melanoma. N Engl J Med. 2015; 372:2521–2532.
Article13. Gadiot J, Hooijkaas AI, Kaiser AD, van Tinteren H, van Boven H, Blank C. Overall survival and PD-L1 expression in metastasized malignant melanoma. Cancer. 2011; 117:2192–2201.
Article14. Hino R, Kabashima K, Kato Y, Yagi H, Nakamura M, Honjo T, et al. Tumor cell expression of programmed cell death-1 ligand 1 is a prognostic factor for malignant melanoma. Cancer. 2010; 116:1757–1766.
Article15. Yuan G, Wu L, Li B, An J. Primary malignant melanoma of the cervix: report of 14 cases and review of literature. Oncotarget. 2017; 8:73162–73167.
Article16. Teixeira JC, Salina JR, Teixeira LC, Andrade LA. Primary melanoma of the uterine cervix FIGO stage III B. Sao Paulo Med J. 1998; 116:1778–1780.
Article17. Cantuaria G, Angioli R, Nahmias J, Estape R, Penalver M. Primary malignant melanoma of the uterine cervix: case report and review of the literature. Gynecol Oncol. 1999; 75:170–174.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case report of Primary Malignant Melanoma of the Uterine Cervix
- A Case of Primary Malignant Melanoma of Uterine Cervix
- Primary amelanotic melanoma of the cervix: case report with review of literature
- Primary malignant melanoma of the uterine cervix: A case report
- A Case of Primary Malignant Melanoma of the Vagina: Vulvovaginal Reconstruction Using Gracilis My ocutaneous Flap Afer Radical Surgery
