Clinical and MRI Characteristics of Uterine Cervical Adenocarcinoma: Its Variants and Mimics
- Affiliations
-
- 1Department of Radiology, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan. saida_sasaki_tsukasa@yahoo.co.jp
- 2Department of Diagnostic Pathology, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan.
- 3Department of Diagnostic Imaging, The Cancer Institute Hospital Japanese Foundation for Cancer Research, Tokyo, Japan.
- 4Department of Obstetrics and Gynecology, Faculty of Medicine, University of Tsukuba, Tsukuba, Japan.
- KMID: 2438266
- DOI: http://doi.org/10.3348/kjr.2018.0458
Abstract
- Adenocarcinoma currently accounts for 10-25% of all uterine cervical carcinomas and has a variety of histopathological subtypes. Among them, mucinous carcinoma gastric type is not associated with high-risk human papillomavirus (HPV) infection and a poor prognosis, while villoglandular carcinoma has an association with high-risk HPV infection and a good prognosis. They show relatively characteristic imaging findings which can be suggested by magnetic resonance imaging (MRI), though the former is sometimes difficult to be distinguished from lobular endocervical glandular hyperplasia. Various kinds of other tumors including squamous cell carcinoma should be also differentiated on MRI, while it is currently difficult to distinguish them on MRI, and HPV screening and pathological confirmation are usually necessary for definite diagnosis and further patient management.
Keyword
MeSH Terms
Figure
-
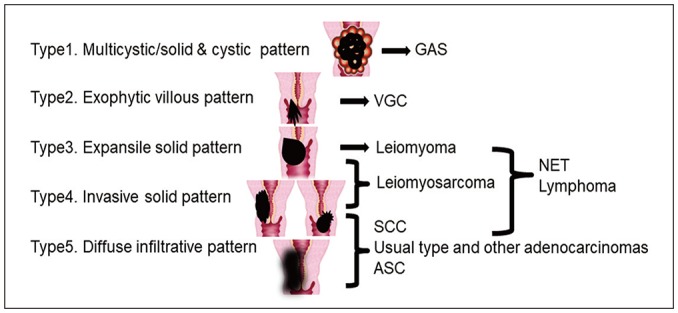
Fig. 1 MRI patterns of different cervical tumors.ASC = adenosquamous carcinoma, GAS = mucinous carcinoma gastric type, MRI = magnetic resonance imaging, NET = neuroendocrine tumor, SCC = squamous cell carcinoma, VGC = villoglandular carcinoma
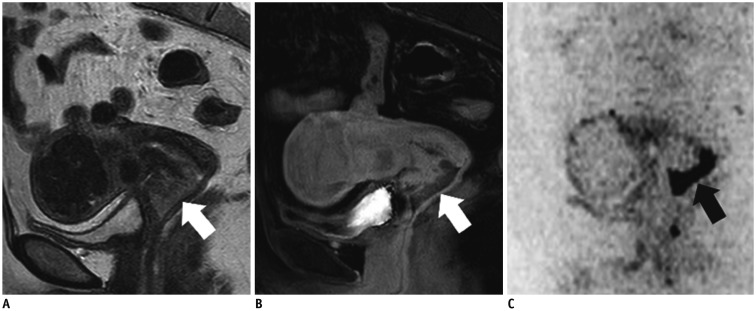
Fig. 2 56-year-old woman with endocervical adenocarcinoma, usual type.A. Sagittal T2WI shows exophytic tumor (protruding inside canal) in cervical lip (arrow) and indicates invasive solid pattern (Fig. 1; Type 4). This is typical pattern for usual type adenocarcinoma. B. Sagittal contrast-enhanced fat-saturated T1WI shows weak enhancement of tumor (arrow). C. Sagittal DWI shows marked restricted diffusion (arrow). DWI = diffusion-weighted imaging, T1WI = T1-weighted imaging, T2WI = T2-weighted imaging
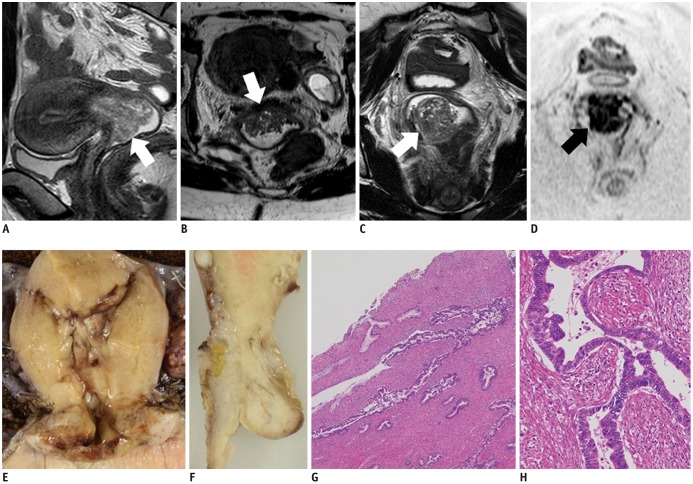
Fig. 3 30-year-old woman with endocervical adenocarcinoma, usual type.A. Sagittal T2WI shows exophytic tumor (arrow) in uterine cervix. Axial (B) and coronal (C) T2WIs show similar to fern leaf-like appearance, i.e., exophytic villous pattern (arrows) (Fig. 1; Type 2). D. Coronal DWI shows restricted diffusion (arrow). E, F. Fixed samples (E, coronal; F, sagittal) show diffuse enlargement of cervix, with invasive solid and diffuse infiltrative pattern, not exophytic villous pattern. G, H. On microscopic examination (G, hematoxylin-eosin staining, original magnification, × 40; H, hematoxylin-eosin staining, original magnification, × 200), tumor shows papillary surface, although it is composed of stromal hyperplasia caused by inflammation. Tumor cell glandules exist in inner part and show concave shape. Pseudostratification and necrotic debris within gland space are typical features of endocervical adenocarcinoma, usual type. Coexistence with CIN also indicates correlation with human papilloma virus infection. CIN = cervical intraepithelial neoplasia
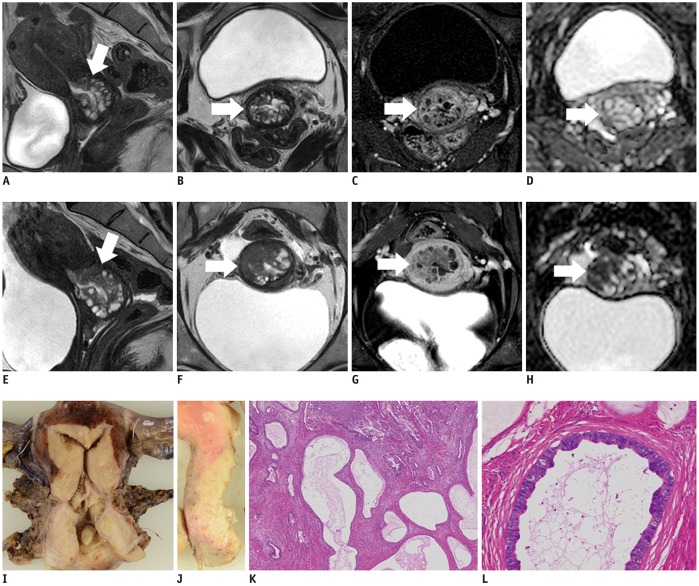
Fig. 4 46-year-old woman with GAS (A–D: 1 year prior).A, E. Sagittal T2WIs show multicystic mass with solid components (arrows) that increases in size. B, F. Axial T2WIs show solid components that have increased in size over year (arrows). Solid and cystic (Fig. 1; Type 1) as well as invasive solid patterns (Fig. 1; Type 4) are seen in this tumor. C, G. Axial contrast-enhanced fat-saturated T1WIs show mild enhancement of solid components (arrows). D, H. Restricted diffusion becomes clear on axial ADC map (arrows) over a year. I, J. Fixed samples (I, coronal; J, sagittal) show solid tumor with multiple cystic components. K. Microscopic examination (hematoxylin-eosin staining, original magnification, × 40) shows tumor cells diffusely infiltrating and involving glandules of LEGH lesion, while maintaining its glandular cavities. L. Microscopic examination (hematoxylin-eosin staining, original magnification, × 200) shows tumor cells with abundant clear cytoplasm. p16 negativity indicated lack of correlation with human papilloma virus infection (not displayed), which is characteristic of GAS. ADC = apparent diffusion coefficient, LEGH = lobular endocervical glandular hyperplasia
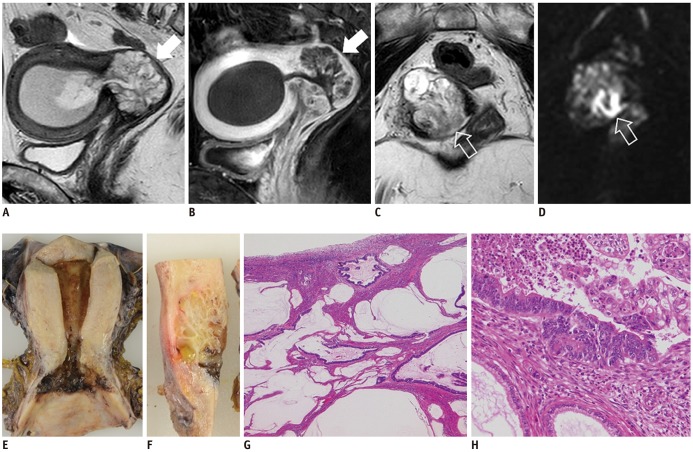
Fig. 5 56-year-old woman with GAS.A. Sagittal T2WI shows multicystic mass (arrow) in uterine cervix, consistent with Type 1 appearance (Fig. 1). B. Sagittal contrast-enhanced fat-saturated T1WI shows well enhanced septa in multicystic mass (arrow). C. Axial T2WI shows core-like hypointense lesion in center of multicystic mass (void arrow). D. Axial DWI shows restricted diffusion in solid core (void arrow), and solid component with restricted diffusion suggests GAS occurring in LEGH lesion. E, F. Fixed samples (E, coronal; F, sagittal) show multicystic tumor in uterine cervix. G, H. Microscopic examination (G, hematoxylin-eosin staining, original magnification, × 40; H, hematoxylin-eosin staining, original magnification, × 200) shows tumor composed of abundant mucinous lakes. Cluster of tumor cells exist in core, and tumor cells are widely spread to line mucinous lakes. p16 negativity indicated lack of correlation with human papilloma virus infection (not displayed).
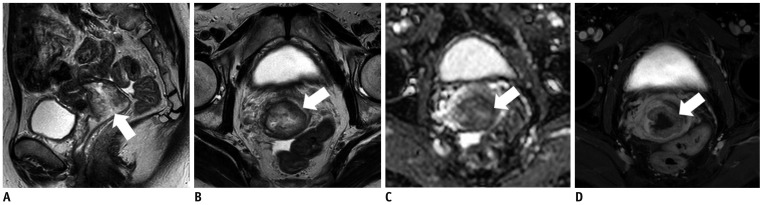
Fig. 6 57-year-old woman with mucinous carcinoma, intestinal type.Sagittal (A) and axial (B) T2WIs show high signal-intensity mass with invasive solid pattern (Fig. 1; Type 4) in uterine cervix (arrows). C. Tumor shows weak restricted diffusion on axial ADC map (arrow). Relatively high signal intensities on T2WI and weak restricted diffusion seem to reflecting intracellular mucinous components. D. Tumor is mildly enhanced on axial contrast-enhanced fat-saturated T1WI (arrow).
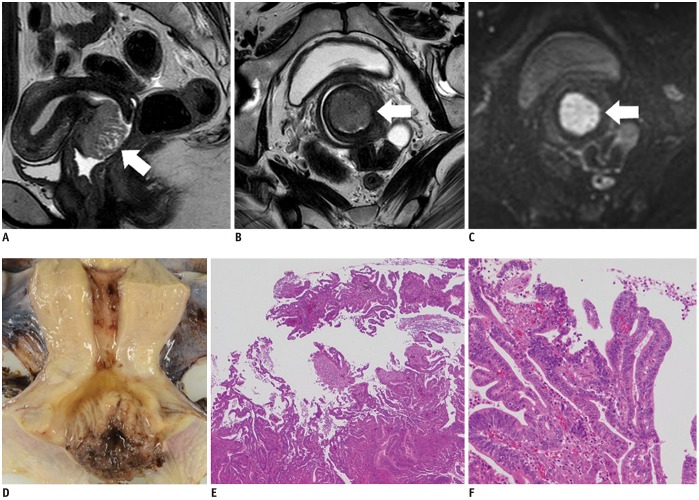
Fig. 7 36-year-old woman with villoglandular carcinoma.Sagittal (A) and axial (B) T2WIs show cervical tumor with fern leaf-like appearance (exophytic villous pattern, Fig. 1; Type 2) (arrows). C. On axial DWI, tumor shows restricted diffusion (arrow), and malignancy is suggested. D. Fixed sample shows cervical tumor with fern leaf-like appearance. E, F. Microscopic examination (E, hematoxylin-eosin staining, original magnification, × 40; F, hematoxylin-eosin staining, original magnification, × 20) shows exophytic tumor with villous fronds lined by well-differentiated tumor cells. Coexistence with CIN also indicates correlation of this tumor with human papilloma virus infection.
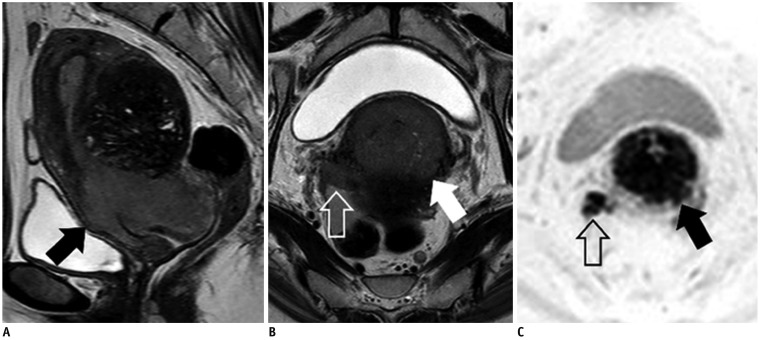
Fig. 8 53-year-old woman with clear cell carcinoma.Sagittal (A) and axial (B) T2WIs show invasive solid tumor (Fig. 1; Type 4) in uterine cervix (arrows) with right parametrial invasion reaching pelvic wall (void arrow). C. On axial DWI, tumor (arrow) and parametrical invasion (void arrow) both show restricted diffusion. It is difficult to distinguish clear cell carcinoma from SCC and endocervical adenocarcinoma, usual type, by MRI alone.
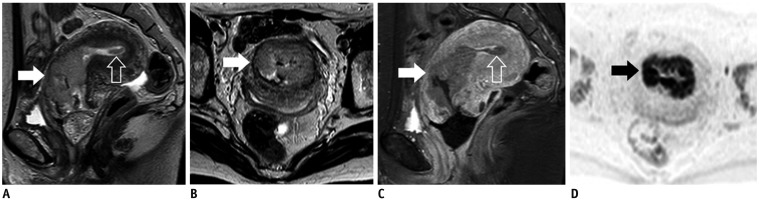
Fig. 9 47-year-old woman with endometrioid carcinomaSagittal (A) and axial (B) T2WIs show invasive solid tumor (Fig. 1; Type 4) mainly located in cervical canal (arrows). Small tumor is also present in uterine corpus (void arrow). C. Sagittal contrast-enhanced fat-saturated T1WI shows mild enhancement of both tumors (arrow, void arrow). D. On axial DWI, tumor shows restricted diffusion (arrow). Pathological diagnosis was uterine corpus carcinoma, stage II, but final clinical diagnosis, which was based on main tumor location, was uterine cervical endometrioid carcinoma, stage IB2, with dissemination in uterine body cavity.
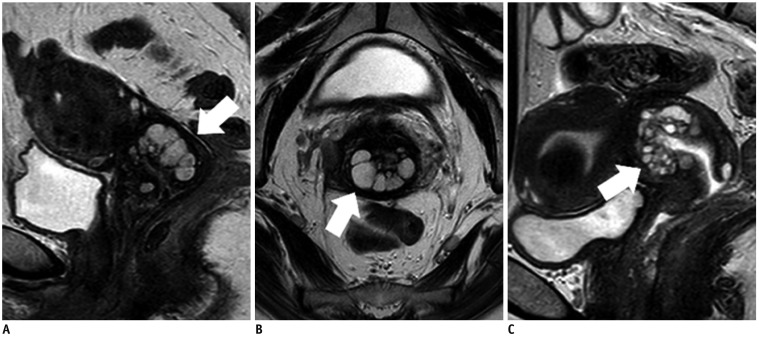
Fig. 10 45-year-old woman with cosmos pattern LEGH (A, B) and 47-year-old woman with microcystic pattern LEGH (C).Sagittal (A) and axial (B) T2WIs show multicystic lesion in uterine cervix (arrows) with Type 1 appearance (Fig. 1). Microcytic parts surrounded by medium-sized to large cysts, indicating cosmos pattern. C. Sagittal T2WI shows multicystic lesion in uterine cervix (arrow) (Fig. 1; Type 1). Aggregation of small cysts without peripheral large cysts, indicating microcystic pattern.
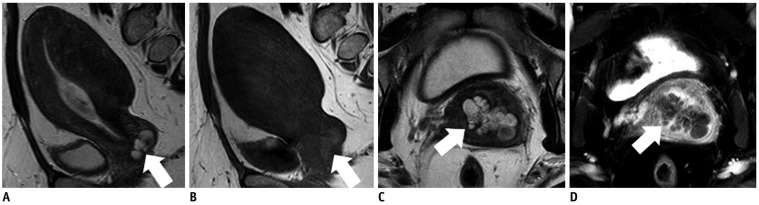
Fig. 11 45-year-old woman with Nabothian cyst.A. Sagittal T2WI shows multicystic lesion near surface of cervical lip (arrow). B. On axial T1WI, cysts show slightly high signal intensity (arrow). C. On axial T2WI, cysts show high to intermediate signal intensity (arrow). Intermediate signal intensities on T2WI and slightly high signal intensities on T1WI indicate mucus contents, and this is characteristic imaging finding of Nabothian cysts. D. There is no enhanced solid component in cysts (arrow) on axial contrast-enhanced fat-saturated T1WI.
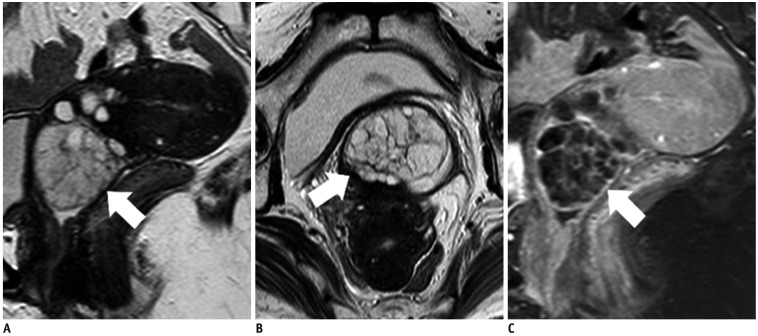
Fig. 12 53-year-old woman with cervical polyp.Sagittal (A) and axial (B) T2WIs show exophytic, oval, multicystic lesion protruding from cervix into vagina (arrows). C. Sagittal contrast-enhanced fat-saturated T1WI shows well-enhanced septa in multicystic lesion (arrow). Fibrovascular core is not clear; therefore, it is difficult to distinguish cervical polyp from LEGH in this case.
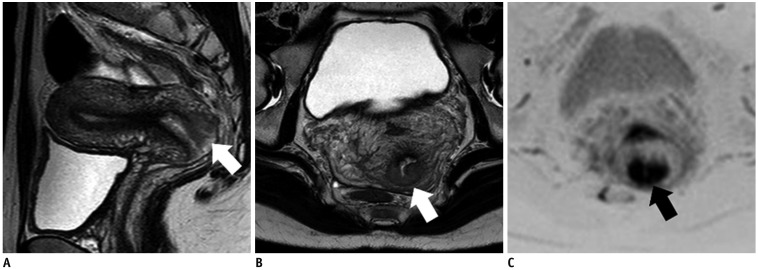
Fig. 13 30-year-old woman with ASC.Sagittal (A) and axial (B) T2WIs show invasive solid tumor (Fig. 1; Type 4) located in posterior cervical lip (arrows). C. Axial DWI shows markedly restricted diffusion (arrow). It is difficult to distinguish ASC from SCC and endocervical adenocarcinoma, usual type.
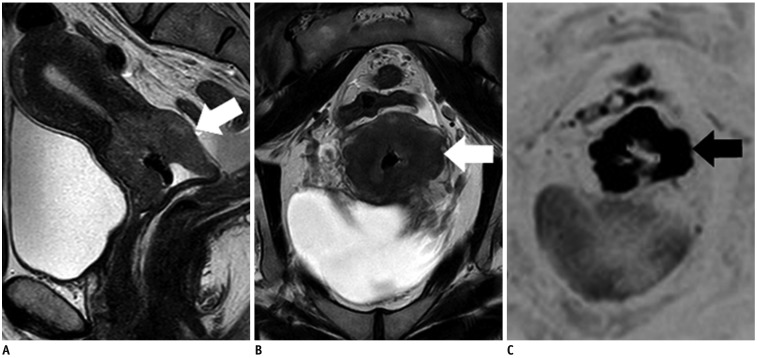
Fig. 14 63-year-old woman with large cell neuroendocrine carcinoma.Sagittal (A) and axial (B) T2WIs show invasive solid tumor (Fig. 1; Type 4) in uterine cervix (arrows). C. Axial DWI shows markedly restricted diffusion (arrow). This lesion is also difficult to distinguish from SCC and endocervical adenocarcinoma, usual type.
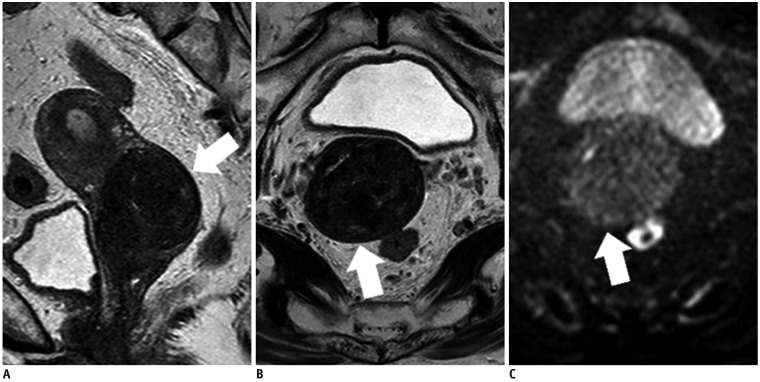
Fig. 15 70-year-old woman with leiomyoma.Sagittal (A) and axial (B) T2WIs show well-defined, homogeneous, hypointense mass (Fig. 1; Type 3) in stroma of uterine cervix (arrows). C. Axial DWI does not show restricted diffusion (arrow).
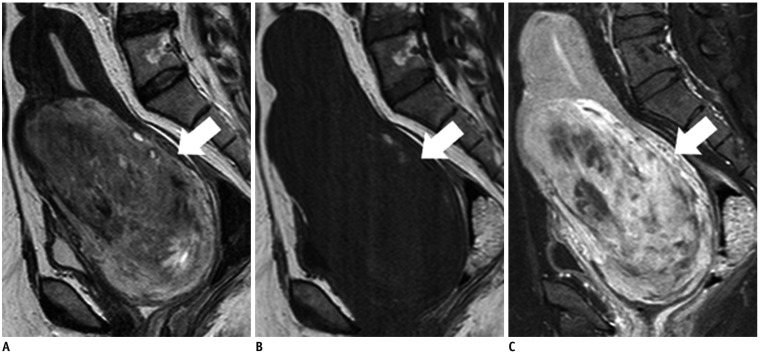
Fig. 16 50-year-old woman with leiomyosarcoma.A. Sagittal T2WI shows invasive solid tumor (Fig. 1; Type 4) in myometrium of uterine cervix (arrow), with relatively high signal intensity. B. Sagittal T1WI shows foci of high signal intensity in tumor (arrow), which are considered to be hemorrhagic foci. C. Heterogeneous enhancement is seen in tumor (arrow) on sagittal contrast-enhanced fat-saturated T1WI. Nonenhanced areas indicate tumor necrosis with hemorrhage.
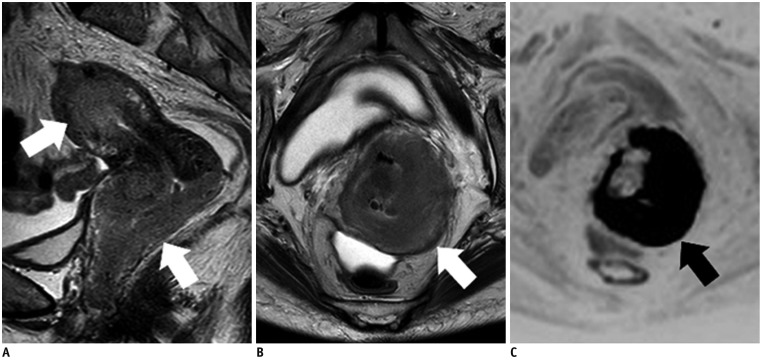
Fig. 17 63-year-old woman with primary lymphoma of uterus, diffuse large B-cell type.Sagittal (A) and axial (B) T2WIs show infiltrating masses (Fig. 1; Type 5) located in cervix and corpus (arrows). C. Tumors show markedly restricted diffusion (arrow) on axial DWI, suggesting rich cellularity.
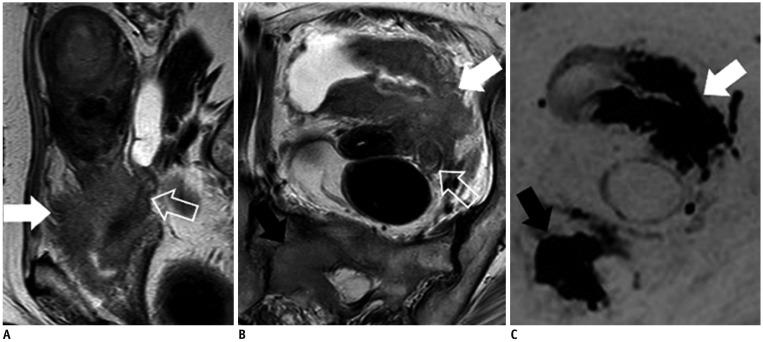
Fig. 18 80-year-old woman with urothelial carcinoma.Sagittal (A) and axial (B) T2WIs show diffuse infiltrating mass (Fig. 1; Type 5) involving bladder (white arrows), left ureter (void arrows), parametrium, and uterine cervix. Bladder is mainly replaced with mass and urothelial carcinoma is speculated by MRI. C. On DWI, main tumor (white arrow) and bone metastasis show restricted diffusion (black arrow). Biopsy specimen from bladder shows urothelial carcinoma, which pathologically suggests that uterine cervix is secondarily involved by bladder cancer.
Reference
-
1. Wilbur DC, Mikami Y, Colgan TJ, Park KJ, Ferenczy AS, Ronnett BM, et al. Tumours of the uterine cervix: glandular tumours and precursors. In : Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2013. p. 183–192.2. Smith HO, Tiffany MF, Qualls CR, Key CR. The rising incidence of adenocarcinoma relative to squamous cell carcinoma of the uterine cervix in the United States--a 24-year population-based study. Gynecol Oncol. 2000; 78:97–105. PMID: 10926787.
Article3. Nogueira-Rodrigues A, Ferreira CG, Bergmann A, de Aguiar SS, Thuler LC. Comparison of adenocarcinoma (ACA) and squamous cell carcinoma (SCC) of the uterine cervix in a sub-optimally screened cohort: a population-based epidemiologic study of 51,842 women in Brazil. Gynecol Oncol. 2014; 135:292–296. PMID: 25130677.
Article4. Kong CS, McCluggage WG. Cervix. In : Mills SE, Greenson JK, Hornick JL, Longacre TA, Reuter VE, editors. Sternberg's diagnostic surgical pathology (Vol. 2). 6th ed. Philadelphia, PA: Wolters Kluwer Health;2015. p. 2419–2426.5. Stolnicu S, Barsan I, Hoang L, Patel P, Terinte C, Pesci A, et al. International Endocervical Adenocarcinoma Criteria and Classification (IECC): a new pathogenetic classification for invasive adenocarcinomas of the endocervix. Am J Surg Pathol. 2018; 42:214–226. PMID: 29135516.6. Zhou J, Wu SG, Sun JY, Li FY, Lin HX, Chen QH, et al. Comparison of clinical outcomes of squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma of the uterine cervix after definitive radiotherapy: a population-based analysis. J Cancer Res Clin Oncol. 2017; 143:115–122. PMID: 27646608.
Article7. Noh JM, Park W, Kim YS, Kim JY, Kim HJ, Kim J, et al. Comparison of clinical outcomes of adenocarcinoma and adenosquamous carcinoma in uterine cervical cancer patients receiving surgical resection followed by radiotherapy: a multicenter retrospective study (KROG 13-10). Gynecol Oncol. 2014; 132:618–623. PMID: 24486605.
Article8. Epstein E, Di Legge A, Måsbäck A, Lindqvist PG, Kannisto P, Testa AC. Sonographic characteristics of squamous cell cancer and adenocarcinoma of the uterine cervix. Ultrasound Obstet Gynecol. 2010; 36:512–516. PMID: 20336641.
Article9. Kidd EA, Siegel BA, Dehdashti F, Grigsby PW. The standardized uptake value for F-18 fluorodeoxyglucose is a sensitive predictive biomarker for cervical cancer treatment response and survival. Cancer. 2007; 110:1738–1744. PMID: 17786947.
Article10. Mitchell DG, Snyder B, Coakley F, Reinhold C, Thomas G, Amendola M, et al. Early invasive cervical cancer: tumor delineation by magnetic resonance imaging, computed tomography, and clinical examination, verified by pathologic results, in the ACRIN 6651/GOG 183 intergroup study. J Clin Oncol. 2006; 24:5687–5694. PMID: 17179104.
Article11. Kido A, Mikami Y, Koyama T, Kataoka M, Shitano F, Konishi I, et al. Magnetic resonance appearance of gastric-type adenocarcinoma of the uterine cervix in comparison with that of usual-type endocervical adenocarcinoma: a pitfall of newly described unusual subtype of endocervical adenocarcinoma. Int J Gynecol Cancer. 2014; 24:1474–1479. PMID: 25188888.
Article12. Shimada M, Kigawa J, Nishimura R, Yamaguchi S, Kuzuya K, Nakanishi T, et al. Ovarian metastasis in carcinoma of the uterine cervix. Gynecol Oncol. 2006; 101:234–237. PMID: 16300819.
Article13. Ando H, Miyamoto T, Kashima H, Takatsu A, Ishii K, Fujinaga Y, et al. Usefulness of a management protocol for patients with cervical multicystic lesions: a retrospective analysis of 94 cases and the significance of GNAS mutation. J Obstet Gynaecol Res. 2016; 42:1588–1598. PMID: 27718288.
Article14. Li H, Sugimura K, Okizuka H, Yoshida M, Maruyama R, Takahashi K, et al. Markedly high signal intensity lesions in the uterine cervix on T2-weighted imaging: differentiation between mucin-producing carcinomas and nabothian cysts. Radiat Med. 1999; 17:137–143. PMID: 10399782.15. Zhao L, Xu T, Cui M, Fu Z. A retrospective review of 11 cases of villoglandular papillary adenocarcinoma of the uterine cervix and a review of the literature. Oncol Lett. 2016; 11:2164–2168. PMID: 26998142.
Article16. Takeuchi M, Matsuzaki K, Bando Y, Sakaki M, Furumoto H, Harada M. Magnetic resonance manifestations of villoglandular papillary adenocarcinoma of the uterine cervix with a fern-leaf-like appearance. Magn Reson Med Sci. 2014; 13:267–270. PMID: 24990463.
Article17. Okamoto Y, Tanaka YO, Nishida M, Tsunoda H, Yoshikawa H, Itai Y. MR imaging of the uterine cervix: imaging-pathologic correlation. Radiographics. 2003; 23:425–445. quiz 534-535. PMID: 12640157.
Article18. Colgan TJ, Kim KR, Hirschowitz L, McCluggage WG. Tumours of the uterine cervix: other epithelial tumours. In : Colgan TJ, Kim KR, Hirschowitz L, McCluggage WG, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2013. p. 194.19. Colgan TJ, Kim I, Hirschowitz L, McCluggage WG. Tumours of the uterine cervix: neuroendocrine tumours. In : Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2013. p. 196–198.20. Lin Y, Lin WY, Liang JA, Lu YY, Wang HY, Tsai SC, et al. Opportunities for 2-[18F] fluoro-2-deoxy-D-glucose PET/CT in cervical-vaginal neuroendocrine carcinoma: case series and literature review. Korean J Radiol. 2012; 13:760–770. PMID: 23118575.21. Duan X, Ban X, Zhang X, Hu H, Li G, Wang D, et al. MR imaging features and staging of neuroendocrine carcinomas of the uterine cervix with pathological correlations. Eur Radiol. 2016; 26:4293–4302. PMID: 26995208.
Article22. Nucci MR, Nielsen GP, Carcangiu ML, Oliva E, Quade B. Tumours of the uterine cervix: mesenchymal tumours and tumour-like lesions. In : Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2013. p. 198–199.23. Tanaka YO, Nishida M, Tsunoda H, Okamoto Y, Yoshikawa H. Smooth muscle tumors of uncertain malignant potential and leiomyosarcomas of the uterus: MR findings. J Magn Reson Imaging. 2004; 20:998–1007. PMID: 15558559.
Article24. Sato K, Yuasa N, Fujita M, Fukushima Y. Clinical application of diffusion-weighted imaging for preoperative differentiation between uterine leiomyoma and leiomyosarcoma. Am J Obstet Gynecol. 2014; 210:368.e1–368.e8. PMID: 24368137.
Article25. Nucci MR, Ferry JA, Carcangiu ML, Oliva E, Quade B. Tumours of the uterine cervix: lymphoid and myeloid tumours. In : Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2013. p. 205.26. Vang R, Medeiros LJ, Ha CS, Deavers M. Non-Hodgkin's lymphomas involving the uterus: a clinicopathologic analysis of 26 cases. Mod Pathol. 2000; 13:19–28. PMID: 10658906.
Article27. Marín C, Seoane JM, Sánchez M, Ruiz Y, García JA. Magnetic resonance imaging of primary lymphoma of the cervix. Eur Radiol. 2002; 12:1541–1545. PMID: 12042965.
Article28. Nucci MR, Ferry JA, Carcangiu ML, Oliva E, Quade B. Tumours of the uterine cervix: secondary tumours. In : Kurman RJ, Carcangiu ML, Herrington CS, Young RH, editors. WHO classification of tumours of female reproductive organs. 4th ed. Lyon: IARC Press;2013. p. 206.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clear Cell Adenocarcinoma of the Uterine Cervix in a 15-Year-Old Girl: A Case Report
- A case of clear cell carcinoma that is unrelated to diethystilbestrol of the uterine cervix
- Treatment Planning Correction Using MRI in the Radiotherapy of Cervical Cancer
- A Case of Cervical Adenocarcinoma with Pulmonary Metastasis Resembling Miliary Tuberculosis
- Uterine Serous Adenocarcinoma in an Elderly Postmenopausal Woman: Clinically Misdiagnosed as Uterine Cervix Cancer
