Consciousness Recovery by Rituximab after Seizure Control in Cryptogenic New-Onset Refractory Status Epilepticus
- Affiliations
-
- 1Department of Neurology, Gyeongsang National University Changwon Hospital, Gyeongsang National University College of Medicine, Changwon, Korea.
- 2Department of Dermatology, Gyeongsang National University Hospital, Gyeongsang National University College of Medicine, Jinju, Korea.
- 3Department of Neurology and Institute of Health Science, Gyeongsang National University College of Medicine, Jinju, Korea. mnkwon21@daum.net, oykwon@gnu.ac.kr
- 4Department of Neurology, Gyeongsang National University Hospital, Jinju, Korea.
- KMID: 2434842
- DOI: http://doi.org/10.18700/jnc.180066
Abstract
- BACKGROUND
New-onset refractory status epilepticus (NORSE) occurs in people without a history of seizures. In these cases, the seizure causes are unclear, and the seizures are not controlled by standard treatment. Autoimmune encephalitis (AIE) can be a cause of NORSE. Cryptogenic NORSE may be associated with AIE, but antibodies associated with the condition have not yet been identified. Primary immunotherapy may not be effective for AIE. Rituximab has improved the prognosis in some cases.
CASE REPORT
We treated a cryptogenic NORSE patient with a combination of antiepileptic drugs and immunotherapy. On the 13th hospital day, the seizures were controlled, but the patient remained in a coma. The patient rapidly recovered after administration of rituximab started on the 26th hospital day.
CONCLUSION
Rituximab may be helpful for cryptogenic NORSE patients in whom primary immunotherapy controls seizures, but fails to improve consciousness.
Keyword
MeSH Terms
Figure
-
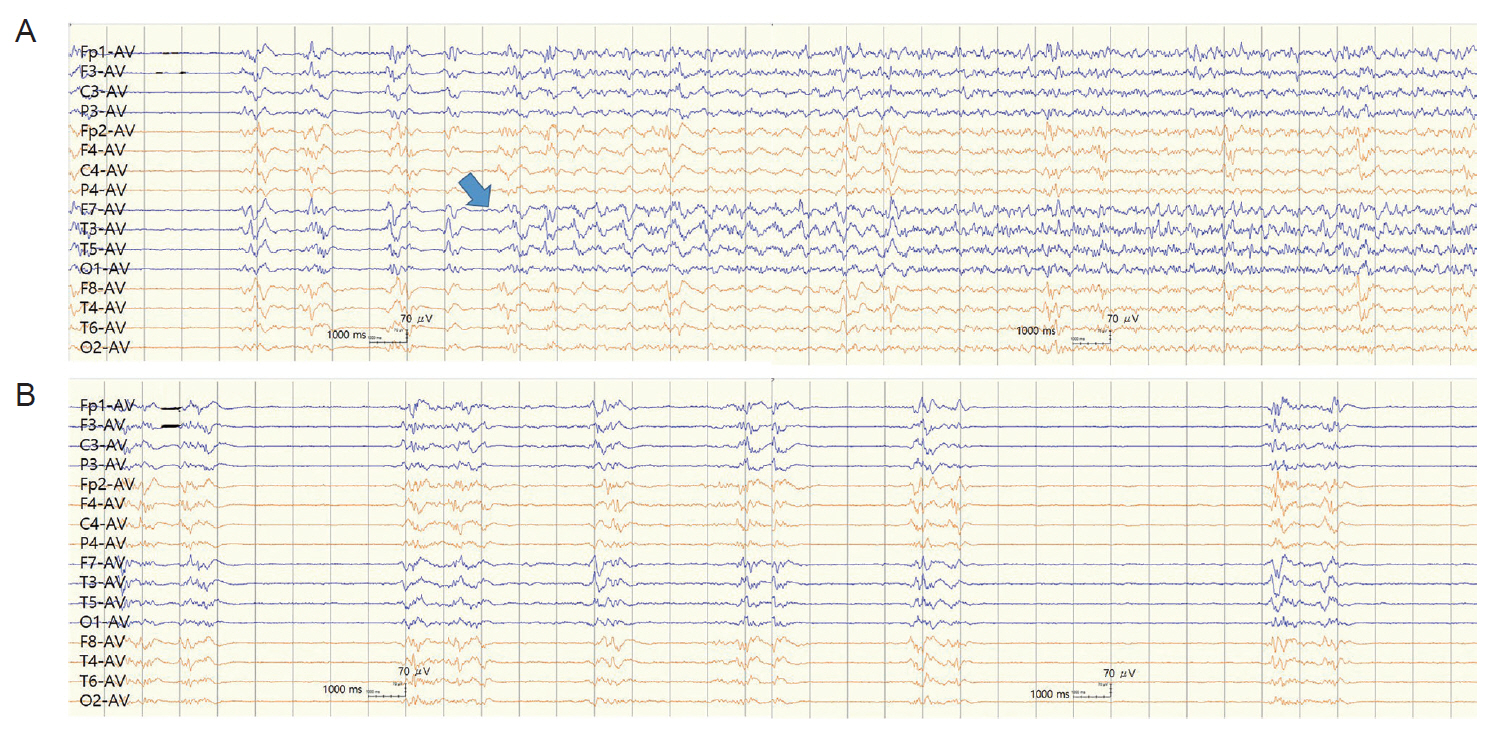
Figure 1. Electroencephalography taken on the 6th hospital day. Electrographic seizures started from the temporal area of the left cerebral hemisphere (filled arrow). Burst suppression patterns preceded the discharges. The ictal discharges propagated to adjacent areas, and sometimes to diffuse areas, including both cerebral hemispheres. Clinical accompaniment was either present or absent (A). The intervals without ictal discharges, when the patient was in status epilepticus, showed burst-suppression patterns (B). AV, average.
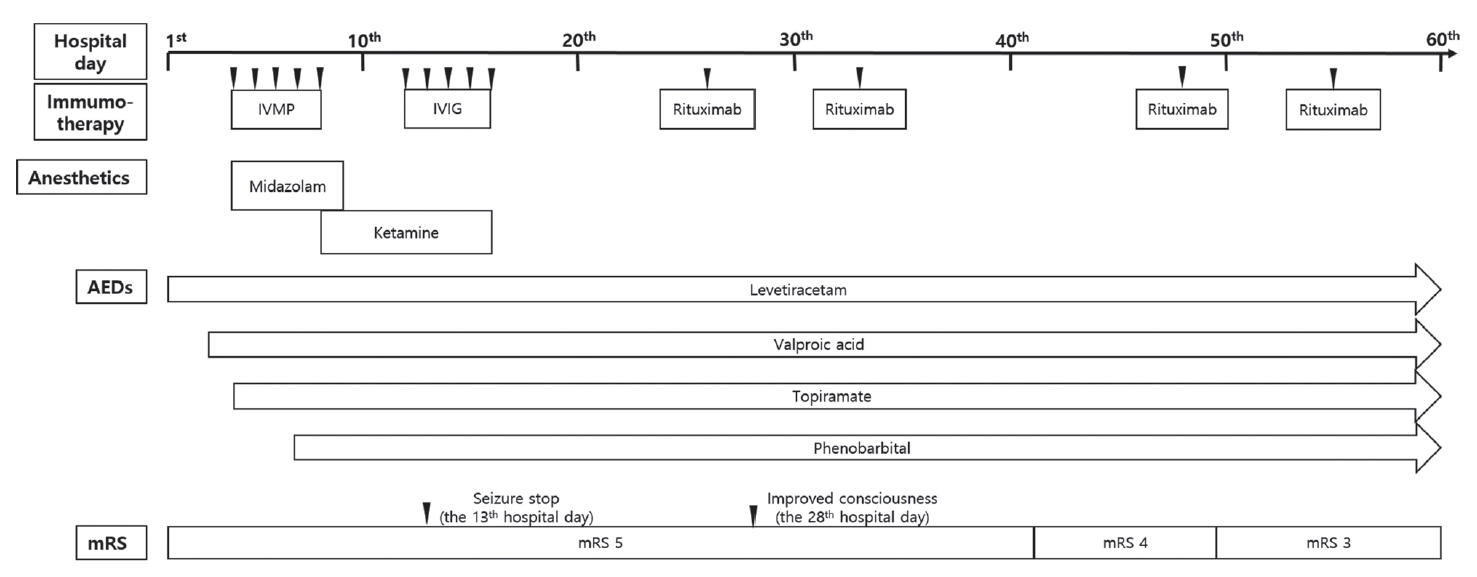
Figure 2. Timeline of hospital course. We treated a cryptogenic NORSE patient with combination therapy, including antiepileptic drugs and primary immunotherapy. On the 13th hospital day, the seizures were controlled, but the patient remained in coma for 10 more days. We started using rituximab on the 24th hospital day. After the administration of rituximab, the patient rapidly regained consciousness. IVMP, intravenous methylprednisolone; IVIG, intravenous immunoglobulin; AEDs, antiepileptic drugs; mRS, modified Rankin Scale; NORSE, new-onset refractory status epilepticus.
Reference
-
1. Gaspard N, Foreman BP, Alvarez V, Cabrera Kang C, Probasco JC, Jongeling AC, et al. New-onset refractory status epilepticus: etiology, clinical features, and outcome. Neurology. 2015; 85:1604–13.2. Gall CR, Jumma O, Mohanraj R. Five cases of new onset refractory status epilepticus (NORSE) syndrome: outcomes with early immunotherapy. Seizure. 2013; 22:217–20.
Article3. Li J, Saldivar C, Maganti RK. Plasma exchange in cryptogenic new onset refractory status epilepticus. Seizure. 2013; 22:70–3.
Article4. Shorvon S, Ferlisi M. The treatment of super-refractory status epilepticus: a critical review of available therapies and a clinical treatment protocol. Brain. 2011; 134(Pt 10):2802–18.
Article5. Wilder-Smith EP, Lim EC, Teoh HL, Sharma VK, Tan JJ, Chan BP, et al. The NORSE (new-onset refractory status epilepticus) syndrome: defining a disease entity. Ann Acad Med Singapore. 2005; 34:417–20.6. Gaspard N, Hirsch LJ, Sculier C, Loddenkemper T, van Baalen A, Lancrenon J, et al. New-onset refractory status epilepticus (NORSE) and febrile infection-related epilepsy syndrome (FIRES): state of the art and perspectives. Epilepsia. 2018; 59:745–52.
Article7. Taylor RP, Lindorfer MA. Drug insight: the mechanism of action of rituximab in autoimmune disease--the immune complex decoy hypothesis. Nat Clin Pract Rheumatol. 2007; 3:86–95.
Article8. Lee WJ, Lee ST, Byun JI, Sunwoo JS, Kim TJ, Lim JA, et al. Rituximab treatment for autoimmune limbic encephalitis in an institutional cohort. Neurology. 2016; 86:1683–91.
Article9. Shin JW, Koo YS, Kim YS, Kim DW, Kim KK, Lee SY, et al. Clinical characterization of unknown/cryptogenic status epilepticus suspected as encephalitis: a multicenter cohort study. J Neuroimmunol. 2018; 315:1–8.
Article10. Iizuka T, Kanazawa N, Kaneko J, Tominaga N, Nonoda Y, Hara A, et al. Cryptogenic NORSE: its distinctive clinical features and response to immunotherapy. Neurol Neuroimmunol Neuroinflamm. 2017; 4:e396.11. Spatola M, Sabater L, Martinez-Hernandez E, Rosenfeld M, Graus F, Dalmau J. Novel findings in autoimmune encephalitis with antibodies against the metabotropic glutamate receptor 5 (mGluR5) (P1.333). Neurology. 2017; 88(16 Supplement):P1–333.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Sevoflurane for the Management of Refractory Status Epilepticus : A case report
- Favorable clinical course after early-intensive immunotherapy for new-onset refractory status epilepticus
- High Dose Intravenous Valproic Acid for the Management of Prolonged Refractory Status Epilepticus : A Case Report of Satisfactory Neurologic Recovery
- Intraoperative refractory status epilepticus caused by propofol -a case report-
- Plasmapheresis for a Female with Cryptogenic New-Onset Refractory Status Epilepticus Not Benefiting from Monoclonal Antibody Therapy
