Modified Tricuspid Annular Plane Systolic Excursion for Assessment of Right Ventricular Systolic Function
- Affiliations
-
- 1Department of Cardiac Anesthesia, Cardiothoracic Centre, CNC, All India Institute of Medical Sciences, Ansari Nagar, New Delhi-110029, INDIA. neetimakhija@hotmail.com
- KMID: 2433761
- DOI: http://doi.org/10.4250/jcvi.2019.27.e8
Abstract
- BACKGROUND
Tricuspid annular plane systolic excursion (TAPSE) has become a popular tool for assessing right ventricular (RV) systolic function because of its ease of application. TAPSE using transesophageal echocardiography (TEE) is limited by alignment with the lateral wall of the RV. Modified TAPSE (m-TAPSE) is a novel method for measuring TAPSE. m-TAPSE is the difference in the "˜apical to lateral tricuspid annulus distance' during diastole and systole. The aim of the present study was to compare prospectively m-TAPSE with the most commonly used parameter TAPSE and near-gold standard 2D echocardiographic parameter RV fractional area change (RV FAC).
METHODS
We conducted a prospective observational study of 125 consecutive patients undergoing coronary artery bypass graft surgery in a single tertiary care center. Post-anesthetic induction TAPSE was recorded using transthoracic echocardiography (TTE). m-TAPSE was recorded using TEE in the mid-esophageal four-chamber view. RV FAC was also assessed using TEE. m-TAPSE < 16 mm, TAPSE < 16 mm and RV FAC < 35% were taken as cut-offs for RV systolic dysfunction. Correlations were assessed using the Pearson correlation coefficient. Sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) were calculated using 2 × 2 cross table.
RESULTS
m-TAPSE was significantly correlated with TAPSE (r = 0.797, p < 0.001). Similarly, a significant correlation was observed between m-TAPSE and RV FAC (r = 0.602, p < 0.001). The sensitivity, specificity, PPV, NPV, and accuracy of m-TAPSE were 100%, 98.3%, 80%, 100% and 98.4%, respectively.
CONCLUSIONS
m-TAPSE correlated well with both RV FAC and TAPSE. Therefore, m-TAPSE can be considered an easily measurable alternative parameter for evaluating RV systolic function in a busy intraoperative setting.
Keyword
MeSH Terms
Figure
-

Figure 1 Measurement of TAPSE. In this figure TAPSE = 2.33 cm. TAPSE: tricuspid annular plane systolic excursion.
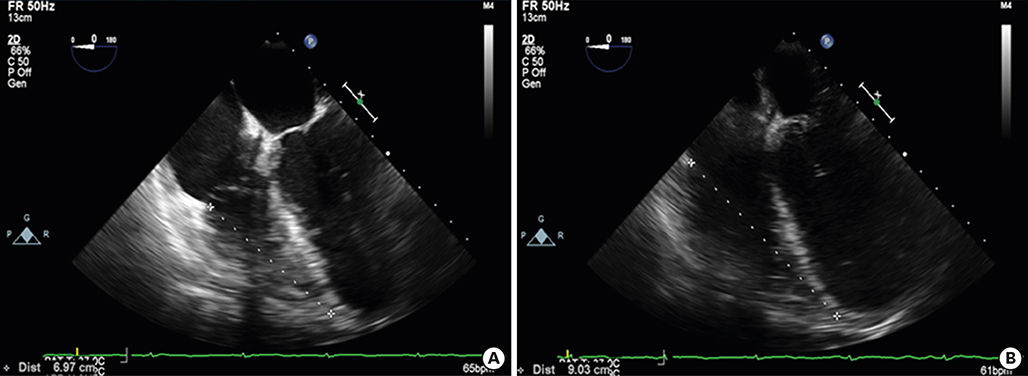
Figure 2 Measurement of m-TAPSE. m-TAPSE was measured as the difference in ‘apical to lateral tricuspid annulus distance’ during systole (A) showing the minimum dimension and diastole (B) showing the maximum dimension on the mid-esophageal four-chamber view. In this figure, m-TAPSE was 9.03-6.97 = 2.06 cm. m-TAPSE: modified tricuspid annular plane systolic excursion.

Figure 3 Mid-esophageal four-chamber view demonstrating RV FAC in diastole (A) and in systole (B). Trabeculation, tricuspid leaflets, and chordae are included in the chamber. In this figure RV FAC = 21.4 - 13.6 / 21.4 × 100 = 36.44%. FAC: fractional area change, RV: right ventricular.
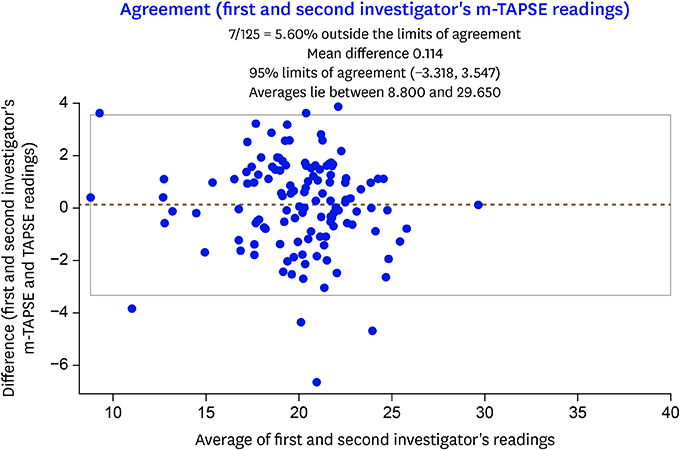
Figure 4 Bland-Altman plot of differences (y-axis) and average of 2 independent observers (x-axis) for m-TAPSE assessment (inter observer variability). m-TAPSE: modified TAPSE, TAPSE: tricuspid annular plane systolic excursion.
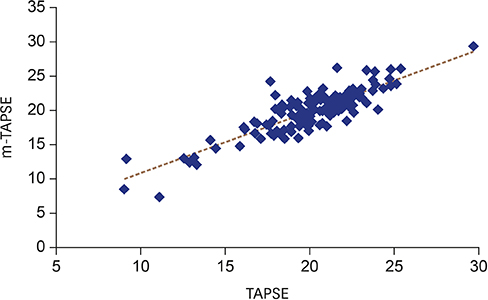
Figure 5 Correlation of TAPSE with m-TAPSE for RV systolic function assessment (correlation coefficient r = 0.797; p < 0.001). m-TAPSE: modified TAPSE, RV: right ventricular, TAPSE: tricuspid annular plane systolic excursion.

Figure 6 Correlation of m-TAPSE with RV FAC for RV systolic function assessment (correlation coefficient r = 0.602; p < 0.001). FAC: fractional area change, m-TAPSE: modified tricuspid annular plane systolic excursion, RV: right ventricular.
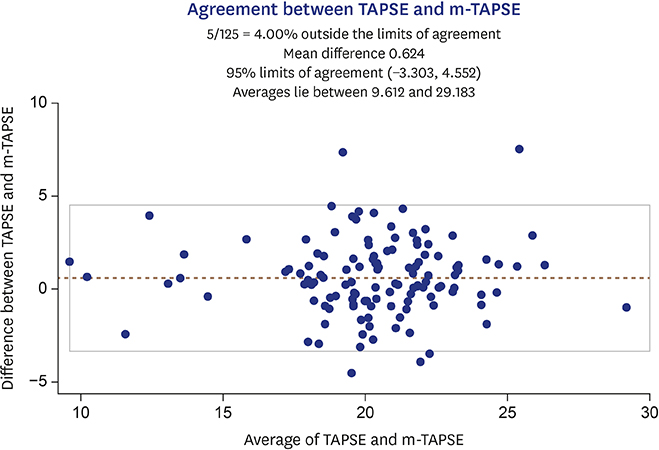
Figure 7 Bland-Altman plot of differences between average values of m-TAPSE and TAPSE. m-TAPSE: modified TAPSE, TAPSE: tricuspid annular plane systolic excursion.
Cited by 1 articles
-
Assessment of Right Ventricular Systolic Function: Conventional Methods and Modified Tricuspid Annular Plane Systolic Excursion
Ji-won Hwang
J Cardiovasc Imaging. 2019;27(1):34-36. doi: 10.4250/jcvi.2019.27.e13.
Reference
-
1. Dell'Italia LJ. The right ventricle: anatomy, physiology, and clinical importance. Curr Probl Cardiol. 1991; 16:653–720.2. Kaul TK, Fields BL. Postoperative acute refractory right ventricular failure: incidence, pathogenesis, management and prognosis. Cardiovasc Surg. 2000; 8:1–9.
Article3. Denault AY, Haddad F, Jacobsohn E, Deschamps A. Perioperative right ventricular dysfunction. Curr Opin Anaesthesiol. 2013; 26:71–81.
Article4. Haddad F, Couture P, Tousignant C, Denault AY. The right ventricle in cardiac surgery, a perioperative perspective: I. Anatomy, physiology, and assessment. Anesth Analg. 2009; 108:407–421.
Article5. Rudski LG, Lai WW, Afilalo J, et al. Guidelines for the echocardiographic assessment of the right heart in adults: a report from the American Society of Echocardiography endorsed by the European Association of Echocardiography, a registered branch of the European Society of Cardiology, and the Canadian Society of Echocardiography. J Am Soc Echocardiogr. 2010; 23:685–713.6. Hu R, Mazer CD, Tousignant C. Relationship between tricuspid annular excursion and velocity in cardiac surgical patients. J Cardiothorac Vasc Anesth. 2014; 28:1198–1202.
Article7. Morita Y, Nomoto K, Fischer GW. Modified tricuspid annular plane systolic excursion using transesophageal echocardiography for assessment of right ventricular function. J Cardiothorac Vasc Anesth. 2016; 30:122–126.
Article8. Miller D, Farah MG, Liner A, Fox K, Schluchter M, Hoit BD. The relation between quantitative right ventricular ejection fraction and indices of tricuspid annular motion and myocardial performance. J Am Soc Echocardiogr. 2004; 17:443–447.
Article9. Maus TM. TAPSE: a red herring after cardiac surgery. J Cardiothorac Vasc Anesth. 2018; 32:779–781.
Article10. Surkova E, Peluso D, Kasprzak JD, Badano LP. Use of novel echocardiographic techniques to assess right ventricular geometry and function. Kardiol Pol. 2016; 74:507–522.
Article11. Horton KD, Meece RW, Hill JC. Assessment of the right ventricle by echocardiography: a primer for cardiac sonographers. J Am Soc Echocardiogr. 2009; 22:776–792.
Article12. Srinivasan C, Sachdeva R, Morrow WR, Greenberg SB, Vyas HV. Limitations of standard echocardiographic methods for quantification of right ventricular size and function in children and young adults. J Ultrasound Med. 2011; 30:487–493.
Article13. Skinner H, Kamaruddin H, Mathew T. Tricuspid annular plane systolic excursion: comparing transthoracic to transesophageal echocardiography. J Cardiothorac Vasc Anesth. 2017; 31:590–594.
Article14. Morita Y, Lencho T, Gunasekaran S, Modak R. Modified tricuspid annular plane systolic excursion using transesophageal echocardiography and its utility to predict postoperative course in heart transplantation and left ventricular assist device implantation. J Cardiothorac Vasc Anesth. 2018; 32:1316–1324.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Assessment of Right Ventricular Systolic Function: Conventional Methods and Modified Tricuspid Annular Plane Systolic Excursion
- Usability consideration about mitral annular plane systolic excursion (MAPSE) and tricuspid annular plane systolic excursion (TAPSE) with point of care ultrasound (POCUS) in emergency: untact pilot experiment before clinically applying them in emergency room
- Evaluation of Right Ventricular Systolic Function by the Analysis of Tricuspid Annular Motion in Patients with Acute Pulmonary Embolism
- Echocardiographic reference z scores of right ventricular dimension and systolic function of children aged 5–12 years
- The Effect of Tonsillectomy and Adenoidectomy on Right Ventricle Function and Pulmonary Artery Pressure by Using Doppler Echocardiography in Children
