Gastric Adenocarcinoma of Fundic Gland Type with Aggressive Transformation and Lymph Node Metastasis: a Case Report
- Affiliations
-
- 1Department of Gastroenterological Surgery, The Cancer Institute Hospital, Japanese Foundation for Cancer Research, Tokyo, Japan. manabu.ohashi@jfcr.or.jp
- 2Department of Pathology, The Cancer Institute Hospital, Japanese Foundation for Cancer Research, Tokyo, Japan.
- 3Division of Pathology, The Cancer Institute, Japanese Foundation for Cancer Research, Tokyo, Japan.
- 4Division of Gastroenterology, Showa University Fujigaoka Hospital, Yokohama, Japan.
- KMID: 2429887
- DOI: http://doi.org/10.5230/jgc.2018.18.e22
Abstract
- A 55-year-old man visited our hospital for a detailed examination of a gastric submucosal tumor that was first detected 10 years prior. The tumor continued to grow and had developed a depressed area in its center. A histopathological examination of biopsy specimens revealed gastric adenocarcinoma of the fundic gland type (GA-FG). It was diagnosed as T2 based on the invasion depth as determined by white-light endoscopy and endoscopic ultrasonography. A total gastrectomy with lymphadenectomy was performed and a GA-FG in the mucosa and submucosa was confirmed histopathologically. However, there was a gradual transition to an infiltrative tubular adenocarcinoma with poorly differentiated components in the muscular and subserosal layers. Metastasis was identified in a dissected lymph node (LN). This is the first report of a GA-FG progressing to an aggressive cancer with LN metastasis. These findings modify our understanding of the pathophysiology of GA-FG.
Keyword
MeSH Terms
Figure
-
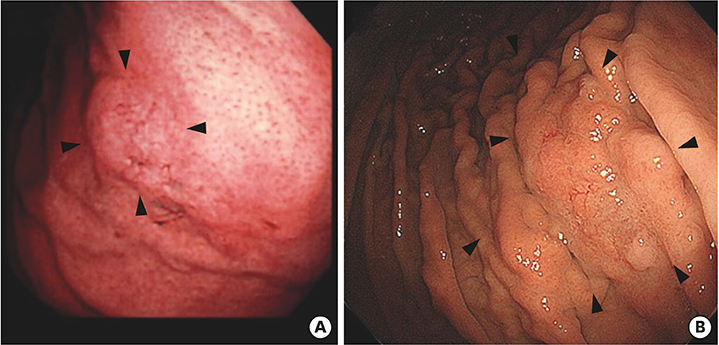
Fig. 1 (A) Gastroscopy findings at the medical check-up during which the tumor was originally detected. (B) Gastroscopy findings 10 years later showing an enlarged submucosal tumor with evident morphological changes (arrows).
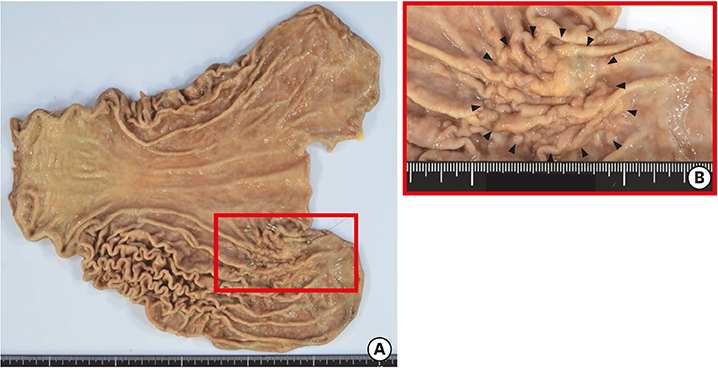
Fig. 2 (A) The resected specimen consists of a locally thickened mass 4.7 cm in diameter located in the posterior wall of the upper gastric body. (B) The lesion borders are indistinct (arrows).
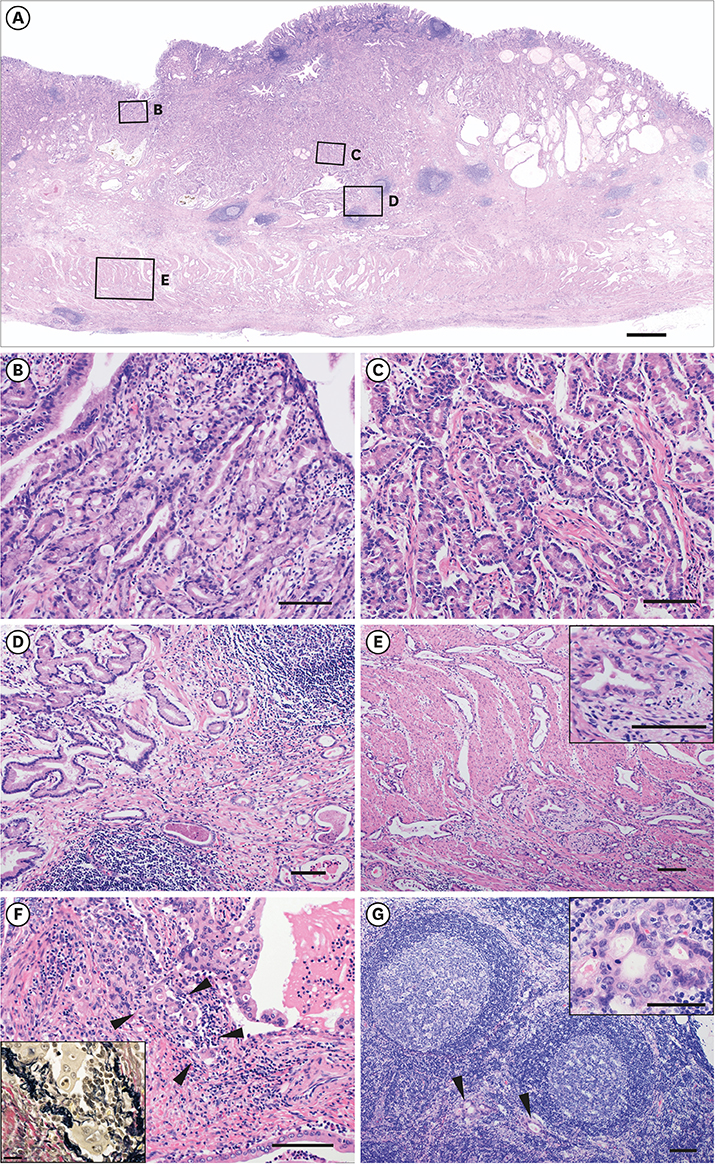
Fig. 3 Representative photomicrographs of gastric adenocarcinoma of the fundic gland type (GA-FG). (A) Low-power image of the tumor. In the top row, four lesions are indicated by squares and labeled B, C, D, and E; these correspond with the images in the bottom row (scale bar: 1 mm). (B) Mucosal and (C) submucosal tumor cells with round nuclei and predominantly basophilic cytoplasm. A few intermingled cells have eosinophilic cytoplasm. (D) Irregularly shaped glands with occasional anastomoses (left) that gradually transition into isolated dilated tubular glands (right). (E) Infiltrative component in the muscular layer. The inset shows neural invasion. (F) Cancer glands exhibiting venous invasion (arrowheads) confirmed by Elastica van Gieson staining. (G) Metastasis in a lymph node (arrowheads). The inset clearly demonstrates the cancer glands. Scale bars of the main images: 100 µm (scale bars of the insets: 50 µm for E, G and 20 µm for F).

Fig. 4 Immunohistochemically stained photomicrographs of cancer components in the mucosa (A-F) and subserosa (G-L). The tumor sections were stained for MUC5AC (B, H), MUC6 (C, I), H+/K+ ATP-ase (D, J), pepsin A (E, K), and Ki-67 (F, L) (scale bars: 50 µm).
Cited by 1 articles
-
Influence of Helicobacter pylori Infection on Endoscopic Findings of Gastric Adenocarcinoma of the Fundic Gland Type
Fumiaki Ishibashi, Keita Fukushima, Takashi Ito, Konomi Kobayashi, Ryu Tanaka, Ryoichi Onizuka
J Gastric Cancer. 2019;19(2):225-233. doi: 10.5230/jgc.2019.19.e21.
Reference
-
1. Ueyama H, Yao T, Nakashima Y, Hirakawa K, Oshiro Y, Hirahashi M, et al. Gastric adenocarcinoma of fundic gland type (chief cell predominant type): proposal for a new entity of gastric adenocarcinoma. Am J Surg Pathol. 2010; 34:609–619.
Article2. Ueyama H, Matsumoto K, Nagahara A, Hayashi T, Yao T, Watanabe S. Gastric adenocarcinoma of the fundic gland type (chief cell predominant type). Endoscopy. 2014; 46:153–157.
Article3. Miyazawa M, Matsuda M, Yano M, Hara Y, Arihara F, Horita Y, et al. Gastric adenocarcinoma of the fundic gland (chief cell-predominant type): a review of endoscopic and clinicopathological features. World J Gastroenterol. 2016; 22:10523–10531.
Article4. Sato Y, Fujino T, Kasagawa A, Morita R, Ozawa SI, Matsuo Y, et al. Twelve-year natural history of a gastric adenocarcinoma of fundic gland type. Clin J Gastroenterol. 2016; 9:345–351.
Article5. Japanese Gastric Cancer Association. Japanese Classification of Gastric Carcinoma. 15th ed. Tokyo: Kanehara Shuppan;2017.6. Kushima R, Sekine S, Matsubara A, Taniguchi H, Ikegami M, Tsuda H. Gastric adenocarcinoma of the fundic gland type shares common genetic and phenotypic features with pyloric gland adenoma. Pathol Int. 2013; 63:318–325.
Article7. Hidaka Y, Mitomi H, Saito T, Takahashi M, Lee SY, Matsumoto K, et al. Alteration in the Wnt/β-catenin signaling pathway in gastric neoplasias of fundic gland (chief cell predominant) type. Hum Pathol. 2013; 44:2438–2448.
Article8. Lewin E, Daroca P, Sikka S, Wu T, Nakanishi Y. Gastric adenocarcinoma of the fundic gland type treated by endoscopic mucosal resection: a case report and review of the literature. Case Rep Pathol. 2016; 2016:8646927.
Article9. Kusumoto C, Shigehara K, Take S, Ishiki K, Taniguchi K. Slow progression of gastric adenocarcinoma of fundic gland type: a case report. Nippon Shokakibyo Gakkai Zasshi. 2016; 113:2042–2049.10. Miyazawa M, Matsuda M, Yano M, Hara Y, Arihara F, Horita Y, et al. Gastric adenocarcinoma of fundic gland type: five cases treated with endoscopic resection. World J Gastroenterol. 2015; 21:8208–8214.
Article11. Terada T. Well differentiated adenocarcinoma of the stomach composed of chief cell-like cells and parietal cells (gastric adenocarcinoma of fundic gland type). Int J Clin Exp Pathol. 2011; 4:797–798.12. Ueo T, Yonemasu H, Ishida T. Gastric adenocarcinoma of fundic gland type with unusual behavior. Dig Endosc. 2014; 26:293–294.
Article13. Reis CA, David L, Nielsen PA, Clausen H, Mirgorodskaya K, Roepstorff P, et al. Immunohistochemical study of MUC5AC expression in human gastric carcinomas using a novel monoclonal antibody. Int J Cancer. 1997; 74:112–121.
Article14. Tanabe H, Iwashita A, Ikeda K, Ohta A, Yao K. Histopathological characteristics of gastric adenocarcinoma of fundic gland type. Stomach Intest. 2015; 50:1469–1479.15. Japanese Gastric Cancer Association. Japanese gastric cancer treatment guidelines 2010 (ver. 3). Gastric Cancer. 2011; 14:113–123.16. Chiba T, Kato K, Masuda T, Ohara S, Iwama N, Shimada T, et al. Clinicopathological features of gastric adenocarcinoma of the fundic gland (chief cell predominant type) by retrospective and prospective analyses of endoscopic findings. Dig Endosc. 2016; 28:722–730.
Article17. Yao T, Ueyama H, Kushima R, Nakajima Y, Hirakawa K, Oshiro Y, et al. New type of gastric carcinoma-adenocarcinoma of the fundic gland type: its clinicopathological features and tumor development. Stomach Intest. 2010; 45:1192–1202.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Gastric Adenocarcinoma of Fundic Gland Type Treated by Endoscopic Submucosal Dissection
- An ovarian mucinous cystadenocarcinoma arising from mature cystic teratoma with para-aortic lymph node metastasis: a case report
- Long-term Observation of Gastric Adenocarcinoma of Fundic Gland Mucosa Type before and after Helicobacter pylori Eradication: a Case Report
- Gastric Adenocarcinoma of Fundic-gland Type Diagnosed and Treated by Endoscopic Mucosal Resection
- M llerian-Type Gland Inclusions in Pelvic Lymph Nodes Mimicking Metastasis: A Case Report and Review of the Literature
