J Rheum Dis.
2018 Oct;25(4):248-254. 10.4078/jrd.2018.25.4.248.
Prevalence of Lower Bone Mineral Density and Its Associated Factors in Korean Children and Adolescents with Juvenile Idiopathic Arthritis
- Affiliations
-
- 1Department of Pediatrics, Hallym University Sacred Heart Hospital, Anyang, Korea. kwangnamkim@naver.com
- KMID: 2429711
- DOI: http://doi.org/10.4078/jrd.2018.25.4.248
Abstract
OBJECTIVE
This study examined the prevalence of low-bone mineral density (BMD) and its associated factors in Korean children and adolescents with juvenile idiopathic arthritis (JIA).
METHODS
Thirty-nine patients with JIA were included in this cross-sectional study. The patients were examined for their bone age (BA) and bone mineral density (BMD). The BMD was measured using dual-energy X-ray absorptiometry on the lumbar spine. Each BMD value was converted to a Z-score by comparing the reference values of the healthy control group in terms of the age and sex of each patient, which was measured using the same device. A Z-score of less than −2.0 was defined as a low BMD. Laboratory tests were performed to detect the serum calcium, phosphorus, alkaline phosphatase, and 25-hydroxyvitamin D levels.
RESULTS
The mean age at the time of the examination was 12.2±3.6 years, and the study comprised a total of 39 patients (16 males, 23 females). Patients with systemic JIA had a lower BMD, which was calculated based on the CA, BA, and HA, than those with non-systemic JIA (P=0.020, P=0.049, and P=0.024, respectively); the corticosteroid user group also showed a lower BMD, which had been calculated based on the CA, BA, and HA, than the corticosteroid non-user group (p=0.002, p=0.022, and p=0.188, respectively).
CONCLUSION
This study suggests that JIA patients have a lower BMD than control subjects. Therefore, treatment, and education are warranted while treating patients with JIA, particularly those requiring oral corticosteroids or those with systemic JIA and appropriate laboratory tests.
MeSH Terms
Figure
-
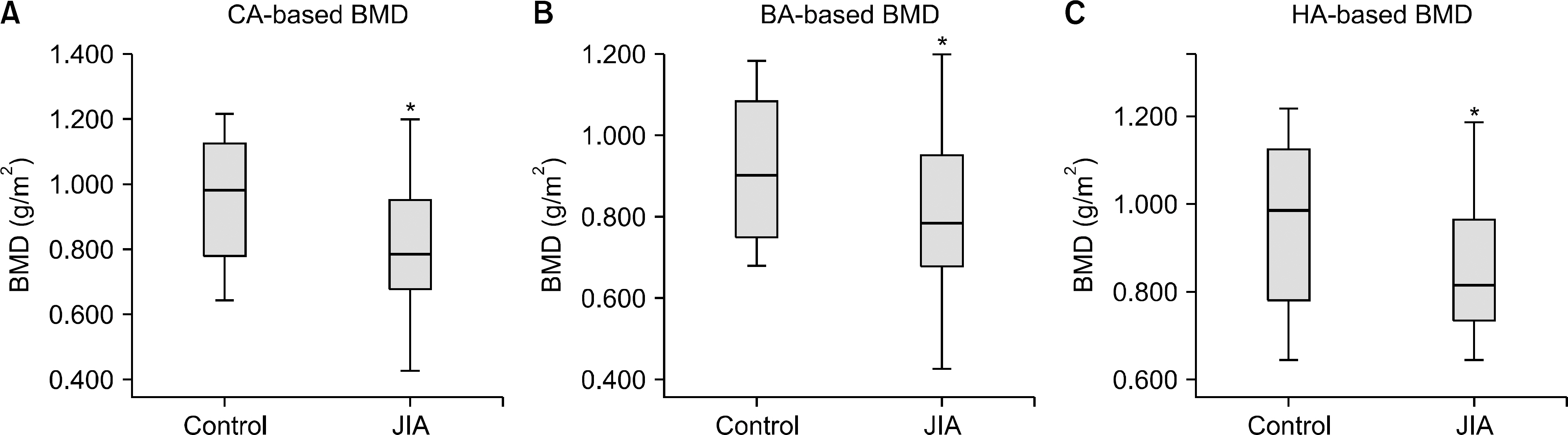
Figure 1. Comparison of BMD between JIA and control group. CA: chronological age, BA: bone age, HA: height age, BMD: bone mineral density, JIA: juvenile idiopathic arthritis. *p-value<0.05.
Reference
-
1. Petty RE, Laxer RM, Lindsley CB, Wedderburn L. Textbook of pediatric rheumatology e-book. Philadelphia (PA): Elsevier Health Sciences;2015.2. Naka H, Iki M, Morita A, Ikeda Y. Effects of pubertal development, height, weight, and grip strength on the bone mineral density of the lumbar spine and hip in peripubertal Japanese children: Kyoto kids increase density in the skeleton study (Kyoto KIDS study). J Bone Miner Metab. 2005; 23:463–9.
Article3. Brabnikova Maresova K. Secondary osteoporosis in patients with juvenile idiopathic arthritis. J Osteoporos. 2011; 2011; 569417.
Article4. McDonagh JE. Osteoporosis in juvenile idiopathic arthritis. Curr Opin Rheumatol. 2001; 13:399–404.
Article5. Masi L, Cimaz R, Simonini G, Bindi G, Stagi S, Gozzini A, et al. Association of low bone mass with vitamin d receptor gene and calcitonin receptor gene polymorphisms in juvenile idiopathic arthritis. J Rheumatol. 2002; 29:2225–31.6. Tortolani PJ, McCarthy EF, Sponseller PD. Bone mineral density deficiency in children. J Am Acad Orthop Surg. 2002; 10:57–66.
Article7. Burnham JM, Shults J, Weinstein R, Lewis JD, Leonard MB. Childhood onset arthritis is associated with an increased risk of fracture: a population based study using the General Practice Research Database. Ann Rheum Dis. 2006; 65:1074–9.
Article8. Huber AM, Ward LM. The impact of underlying disease on fracture risk and bone mineral density in children with rheumatic disorders: A review of current literature. Semin Arthritis Rheum. 2016; 46:49–63.
Article9. Nusman CM, Anink J, Otten MH, van Rossum MA, van Rijn RR, Maas M, et al. Bone health of patients with juvenile idiopathic arthritis: a comparison between dual-energy X-ray absorptiometry and digital X-ray radiogrammetry. Eur J Radiol. 2015; 84:1999–2003.
Article10. Oh YJ, La KS, Rhie YJ, Lee KH, Park SH, Choung JT, et al. Bone mineral density and correlation factors in normal children and adolescence. J Korean Soc Pediatr Endocrinol. 2009; 14:38–44.11. Lim JS. Pediatric dual-energy X-ray absorptiometry: interpretation and clinical and research application. Korean J Pediatr. 2010; 53:286–93.
Article12. Stagi S, Masi L, Capannini S, Cimaz R, Tonini G, Matucci-Cerinic M, et al. Cross-sectional and longitudinal evaluation of bone mass in children and young adults with juvenile idiopathic arthritis: the role of bone mass determinants in a large cohort of patients. J Rheumatol. 2010; 37:1935–43.
Article13. Petty RE, Southwood TR, Manners P, Baum J, Glass DN, Goldenberg J, et al. International League of Associations for Rheumatology classification of juvenile idiopathic arthritis: second revision, Edmonton, 2001. J Rheumatol. 2004; 31:390–2.14. Holick MF. Vitamin D deficiency. N Engl J Med. 2007; 357:266–81.
Article15. Lim JS, Hwang JS, Lee JA, Kim DH, Park KD, Cheon GJ, et al. Bone mineral density according to age, bone age, and pubertal stages in Korean children and adolescents. J Clin Densitom. 2010; 13:68–76.
Article16. Moon JS, Lee SY, Nam CM, Choi JM, Choe BK, Seo JW, et al. 2007 Korean National Growth Charts: review of developmental process and an outlook. Korean J Pediatr. 2008; 51:1–25.
Article17. Henderson CJ, Specker BL, Sierra RI, Campaigne BN, Lovell DJ. Total-body bone mineral content in non-cortico-steroid-treated postpubertal females with juvenile rheumatoid arthritis: frequency of osteopenia and contributing factors. Arthritis Rheum. 2000; 43:531–40.
Article18. Lien G, Flatø B, Haugen M, Vinje O, Sørskaar D, Dale K, et al. Frequency of osteopenia in adolescents with early-onset juvenile idiopathic arthritis: a long-term outcome study of one hundred five patients. Arthritis Rheum. 2003; 48:2214–23.
Article19. Dey S, Jahan A, Yadav TP, Bhagwani DK, Sachdev N. Measurement of bone mineral density by dual energy X-ray absorptiometry in juvenile idiopathic arthritis. Indian J Pediatr. 2014; 81:126–32.
Article20. Hämäläinen H, Arkela-Kautiainen M, Kautiainen H, Haapasaari J, Leirisalo-Repo M. Bone mineral content in young adults with active or inactive juvenile idiopathic arthritis and in controls. Scand J Rheumatol. 2010; 39:219–22.
Article21. Thornton J, Pye SR, O'Neill TW, Rawlings D, Francis RM, Symmons DP, et al. Bone health in adult men and women with a history of juvenile idiopathic arthritis. J Rheumatol. 2011; 38:1689–93.
Article22. Tengstrand B, Larsson E, Klareskog L, Hafström I. Randomized withdrawal of long-term prednisolone treatment in rheumatoid arthritis: effects on inflammation and bone mineral density. Scand J Rheumatol. 2007; 36:351–8.
Article23. Buckley L, Guyatt G, Fink HA, Cannon M, Grossman J, Hansen KE, et al. 2017 American College of Rheumatology Guideline for the Prevention and Treatment of Glucocorti-coid-Induced Osteoporosis. Arthritis Care Res (Hoboken). 2017; 69:1095–110.
Article24. Johnston CC Jr, Miller JZ, Slemenda CW, Reister TK, Hui S, Christian JC, et al. Calcium supplementation and increases in bone mineral density in children. N Engl J Med. 1992; 327:82–7.
Article25. Frost HM, Schönau E. The “muscle-bone unit” in children and adolescents: a 2000 overview. J Pediatr Endocrinol Metab. 2000; 13:571–90.
Article26. Kotaniemi A, Savolainen A, Kröger H, Kautiainen H, Isomäki H. Weight-bearing physical activity, calcium intake, systemic glucocorticoids, chronic inflammation, and body constitution as determinants of lumbar and femoral bone mineral in juvenile chronic arthritis. Scand J Rheumatol. 1999; 28:19–26.27. Lien G, Selvaag AM, Flatø B, Haugen M, Vinje O, Sørskaar D, et al. A two-year prospective controlled study of bone mass and bone turnover in children with early juvenile idiopathic arthritis. Arthritis Rheum. 2005; 52:833–40.
Article28. Pepmueller PH, Cassidy JT, Allen SH, Hillman LS. Bone mineralization and bone mineral metabolism in children with juvenile rheumatoid arthritis. Arthritis Rheum. 1996; 39:746–57.
Article29. Hillman L, Cassidy JT, Johnson L, Lee D, Allen SH. Vitamin D metabolism and bone mineralization in children with juvenile rheumatoid arthritis. J Pediatr. 1994; 124:910–6.
Article30. Islam MF, Islam MI, Talukdar MK, Rahman SA. Bone mineral density in children with juvenile idiopathic arthritis: a hospital based study. Bangladesh J Child Health. 2013; 37:18–21.
Article31. Gordon CM, Leonard MB, Zemel BS. International Society for Clinical Densitometry. 2013 Pediatric Position Development Conference: executive summary and reflections. J Clin Densitom. 2014; 17:219–24.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Bertolotti’s Syndrome Misdiagnosed as Juvenile Idiopathic Arthritis in an Adolescent Girl with Low Back Pain
- Bone Densitometry in Rheumatoid Arthritis
- A Case of Idiopathic Juvenile Osteoporosis
- Role of Biomarkers in Juvenile Idiopathic Arthritis
- Body Mass Index and Bone Mineral Densityin Patients with Adolescent Idiopathic Scoliosis
