The Risk of Rosacea According to Chronic Diseases and Medications: A 5-Year Retrospective, Multi-Institutional Case-Control Study
- Affiliations
-
- 1Department of Dermatology, Hallym University Kangnam Sacred Heart Hospital, College of Medicine, Hallym University, Seoul, Korea. dermap@hanmail.net hyeonekim@gmail.com
- KMID: 2428923
- DOI: http://doi.org/10.5021/ad.2018.30.6.676
Abstract
- BACKGROUND
Rosacea is associated with chronic systemic disease. However, research is lacking in Asian countries.
OBJECTIVE
To evaluate the association between rosacea and cardiovascular diseases (CVDs) related systemic comorbidities, and the use of antihypertensive and antihyperlipidemic drugs in Korea.
METHODS
A five-year retrospective study, using hospital database, was conducted in five medical centers for five years. Totally 1,399,528 patients were evaluated.
RESULTS
The overall frequency for diagnosed rosacea was 0.18% over five years (2,536 rosacea patients). Patients with diabetes and patients with dyslipidemia were more likely to have rosacea (odd ratio [OR] 2.724, 95% confidence interval [CI] 1.295~5.730, p=0.016; OR 1.788, 95% CI 1.445~2.212, p < 0.001). Patients with CVD were less likely to have rosacea (OR 0.431, 95% CI 0.244~0.760, p=0.003). Patients with α-blocker prescriptions and patients with β-blocker prescriptions showed a tendency diagnosed with rosacea frequently (OR 1.963, 95% CI 1.200~3.212, p=0.006; OR 3.939, 95% CI 3.512~4.419, p < 0.001). Patients with [beta]-hydroxy-[beta]-methylglutaryl coenzyme A (HMG-CoA) reductase inhibitor, and those with fibrate, were prone to have rosacea (OR 1.599, 95% CI 1.390~1.839, p < 0.001; OR 1.660, 95% CI 1.056~2.609, p=0.026). As adjusted results, among the patients who took HMG-CoA reductase inhibitor without dyslipidemia, rosacea was less likely to be diagnosed (OR 0.780, 95% CI 0.620~0.982, p=0.034).
CONCLUSION
Rosacea is associated with chronic diseases and drugs.
MeSH Terms
Figure
-
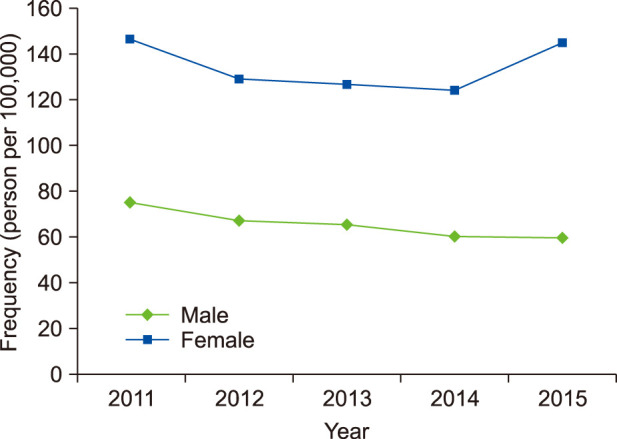
Fig. 1 Changes in the frequency of diagnosed rosacea by sex in five medical centers for five years.
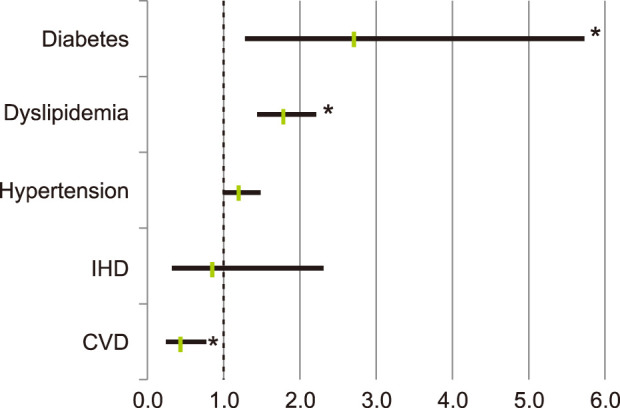
Fig. 2 Risk of diagnosed rosacea according to chronic systemic diseases. IHD: ischemic heart disease, CVD: cardiovascular disease. *p<0.05.
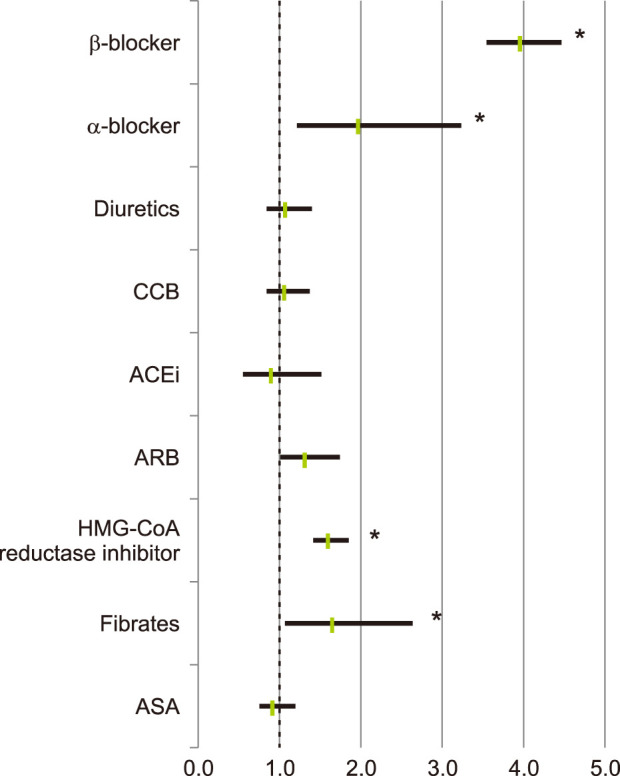
Fig. 3 Risk of diagnosed rosacea in relation to medications such as antihypertensive and antihyperlipidemic drugs. CCB: calcium channel blocker, ACEi: angiotensin-converting-enzyme inhibitor, ARB: angiotensin II receptor blocker, HMG-CoA: [beta]-hydroxy-[beta]-methylglutaryl coenzyme A, ASA: aspirin. *p<0.05.
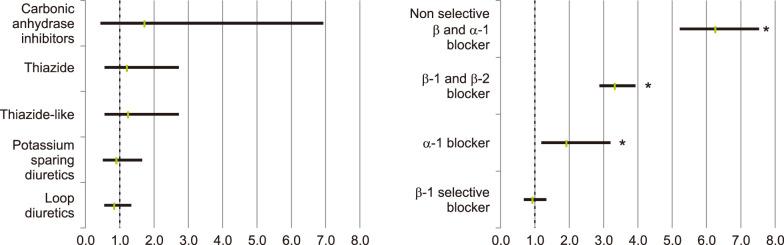
Fig. 4 (A) Risk of diagnosed rosacea according to specific diuretics, (B) risk of diagnosed rosacea according to specific α-blockers and β-blocker, classified drugs by subtypes. *p<0.05.
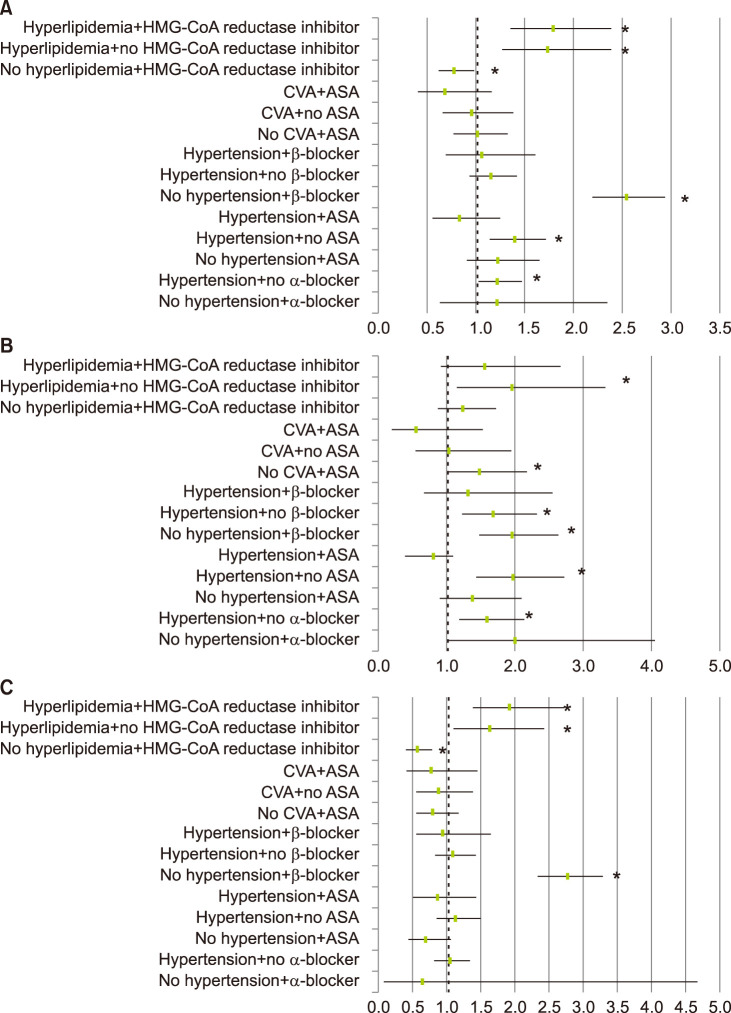
Fig. 5 Odds ratio for the risk of diagnosed rosacea in (A) total population, (B) males, and (C) females, after subdivided analysis. HMG-CoA: [beta]-hydroxy-[beta]-methylglutaryl coenzyme A, CVA: cerebrovascular attack, ASA: aspirin. *p<0.05.
Reference
-
1. Duman N, Ersoy Evans S, Atakan N. Rosacea and cardiovascular risk factors: a case control study. J Eur Acad Dermatol Venereol. 2014; 28:1165–1169. PMID: 23909954.
Article2. Rainer BM, Fischer AH, Luz Felipe da Silva D, Kang S, Chien AL. Rosacea is associated with chronic systemic diseases in a skin severity–dependent manner: results of a case-control study. J Am Acad Dermatol. 2015; 73:604–608. PMID: 26256428.3. Rueda LJ, Motta A, Pabón JG, Barona MI, Meléndez E, Orozco B, et al. Epidemiology of rosacea in Colombia. Int J Dermatol. 2017; 56:510–513. PMID: 28239916.
Article4. Schwab VD, Sulk M, Seeliger S, Nowak P, Aubert J, Mess C, et al. Neurovascular and neuroimmune aspects in the pathophysiology of rosacea. J Investig Dermatol Symp Proc. 2011; 15:53–62.
Article5. Mehta NN, Azfar RS, Shin DB, Neimann AL, Troxel AB, Gelfand JM. Patients with severe psoriasis are at increased risk of cardiovascular mortality: cohort study using the General Practice Research Database. Eur Heart J. 2009; 31:1000–1006. PMID: 20037179.
Article6. Ozbalkan Z, Efe C, Cesur M, Ertek S, Nasiroglu N, Berneis K, et al. An update on the relationships between rheumatoid arthritis and atherosclerosis. Atherosclerosis. 2010; 212:377–382. PMID: 20430394.
Article7. Itani S, Arabi A, Harb D, Hamzeh D, Kibbi AG. High prevalence of metabolic syndrome in patients with psoriasis in Lebanon: a prospective study. Int J Dermatol. 2016; 55:390–395. PMID: 26748974.
Article8. Merticariu A, Marinescu L, Giurcăneanu C. Rosacea and its comorbidities. J Transl Med Res. 2016; 21:17–23.
Article9. Spoendlin J, Voegel JJ, Jick SS, Meier CR. Diabetes mellitus, antidiabetic drugs and the risk of developing rosacea. Pharmacoepidemiol Drug Saf. 2012; 21:275–276.10. Tan J, Schöfer H, Araviiskaia E, Audibert F, Kerrouche N, Berg M. Prevalence of rosacea in the general population of Germany and Russia - the RISE study. J Eur Acad Dermatol Venereol. 2016; 30:428–434. PMID: 26915718.11. Koo BS, Kwon HJ, Kim BC, Lee KS, Song JY. A clinical study of 133 patients with rosacea. Korean J Dermatol. 1997; 35:405–410.12. Kim TH, Hwang SM, Lee WS, Ahn SK, Choi EH. A clinical study of rosacea. Korean J Dermatol. 2000; 38:583–588.13. Kim MS, Kim BS, Koh WS, Lee SS, Seo SL, Chun DK, et al. Rosacea: clinical study of 67 cases. Ann Dermatol. 2001; 13:39–43.14. Libby P, Ridker PM, Maseri A. Inflammation and atherosclerosis. Circulation. 2002; 105:1135–1143. PMID: 11877368.
Article15. Luebberding S, Krueger N, Kerscher M. Skin physiology in men and women: in vivo evaluation of 300 people including TEWL, SC hydration, sebum content and skin surface pH. Int J Cosmet Sci. 2013; 35:477–483. PMID: 23713991.16. BORRIE P. Rosacea with special reference to its ocular manifestations. Br J Dermatol. 1953; 65:458–463. PMID: 13115586.
Article17. Jowkar F, Namazi MR. Statins in dermatology. Int J Dermatol. 2010; 49:1235–1243. PMID: 20964647.
Article18. Namazi MR. Statins: novel additions to the dermatologic arsenal? Exp Dermatol. 2004; 13:337–339. PMID: 15186318.
Article19. McKay A, Leung BP, McInnes IB, Thomson NC, Liew FY. A novel anti-inflammatory role of simvastatin in a murine model of allergic asthma. J Immunol. 2004; 172:2903–2908. PMID: 14978092.
Article20. Stoll LL, McCormick ML, Denning GM, Weintraub NL. Antioxidant effects of statins. Drugs Today (Barc). 2004; 40:975–990. PMID: 15645009.
Article21. Katsumoto M, Shingu T, Kuwashima R, Nakata A, Nomura S, Chayama K. Biphasic effect of HMG-CoA reductase inhibitor, pitavastatin, on vascular endothelial cells and angiogenesis. Circ J. 2005; 69:1547–1555. PMID: 16308507.
Article22. Luan Z, Chase AJ, Newby AC. Statins inhibit secretion of metalloproteinases-1,-2,-3, and -9 from vascular smooth muscle cells and macrophages. Arterioscler Thromb Vasc Biol. 2003; 23:769–775. PMID: 12663370.23. Koh KK, Ahn JY, Jin DK, Han SH, Kim HS, Choi IS, et al. Comparative effects of statin and fibrate on nitric oxide bioactivity and matrix metalloproteinase in hyperlipidemia. Int J Cardiol. 2004; 97:239–244. PMID: 15458690.
Article24. Dollery CM, McEwan JR, Henney AM. Matrix metalloproteinases and cardiovascular disease. Circ Res. 1995; 77:863–868. PMID: 7554139.
Article25. Galis ZS, Khatri JJ. Matrix metalloproteinases in vascular remodeling and atherogenesis: the good, the bad, and the ugly. Circ Res. 2002; 90:251–262. PMID: 11861412.26. Odom R, Dahl M, Dover J, Draelos Z, Drake L, Macsai M, et al. Standard management options for rosacea, part 1: overview and broad spectrum of care. Cutis. 2009; 84:43–47. PMID: 19743724.27. Spoendlin J, Voegel J, Jick S, Meier CR. Antihypertensive drugs and the risk of incident rosacea. Br J Dermatol. 2014; 171:130–136. PMID: 24428524.
Article28. Powell FC. Clinical practice. Rosacea. N Engl J Med. 2005; 352:793–803. PMID: 15728812.29. Natale F, Cirillo C, Granato C, Concilio C, Siciliano A, Credendino M, et al. Worsening of rosacea in patients treated with dihydropyridine calcium channel blockers: a clinical observation. Hypertens Res. 2011; 34:790–791. PMID: 21451527.
Article30. Spoendlin J, Voegel JJ, Jick SS, Meier CR. Risk of rosacea in patients with diabetes using insulin or oral antidiabetic drugs. J Invest Dermatol. 2013; 133:2790–2793. PMID: 23657502.
Article31. Browne D, Meeking D, Shaw K, Cummings M. Review: endothelial dysfunction and pre-symptomatic atherosclerosis in type 1 diabetes — pathogenesis and identification. Br J Diabetes Vasc Dis. 2003; 3:27–34.
Article32. Guarrera M, Parodi A, Cipriani C, Divano C, Rebora A. Flushing in rosacea: a possible mechanism. Arch Dermatol Res. 1982; 272:311–316. PMID: 6219630.
Article
