A composite of urinary biomarkers for differentiating between tubulointerstitial inflammation and interstitial fibrosis/tubular atrophy in kidney allografts
- Affiliations
-
- 1Asan Institute for Life Sciences, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. sshin@amc.seoul.kr
- 2Division of Kidney and Pancreas Transplantation, Department of Surgery, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2427361
- DOI: http://doi.org/10.14701/ahbps.2018.22.4.310
Abstract
- BACKGROUNDS/AIMS
Compared with a single urinary biomarker, a composite of multiple urinary biomarkers may be more helpful for differentiating tubulointerstitial inflammation from interstitial fibrosis/tubular atrophy (IFTA) in kidney allografts.
METHODS
In this cross-sectional cohort study, we collected urine samples from 115 patients with for-cause biopsy, 53 patients with stable allografts, and 50 living kidney donors. We measured the urinary levels of transglutaminase 2 (TG2), syndecan-4 (SDC4), alpha 1 microglobulin (A1M), interferon-inducible protein 10 (IP-10), interleukin 6 (IL-6), and monocyte chemoattractant protein-1 (MCP-1).
RESULTS
The for-cause biopsy group showed significantly higher levels of logeTG2/Cr, logeA1M/Cr, logeIL-6/Cr, and logeMCP-1/Cr compared with other groups. In the for-cause biopsy group, logeTG2/Cr level was positively correlated with the severity of IFTA. After adjusting for age, sex, body mass index, diabetes, hypertension, cardiovascular disease, and the interval between kidney transplant and biopsy, TG2 and the interval between transplant and biopsy were significantly correlated variables for the severity of IFTA. Regarding tubulointerstitial inflammation, Body mass index, TG2, SDC4, and IP-10 were positively-correlated variables, and MCP-1 and the interval between transplant and biopsy were negatively-correlated variables.
CONCLUSIONS
Our results show that post-transplant urinary levels of TG2, SDC4, MCP-1 and IP-10 may be a useful biomarker for tubulointerstitial inflammation and IFTA.
Keyword
MeSH Terms
Figure
-
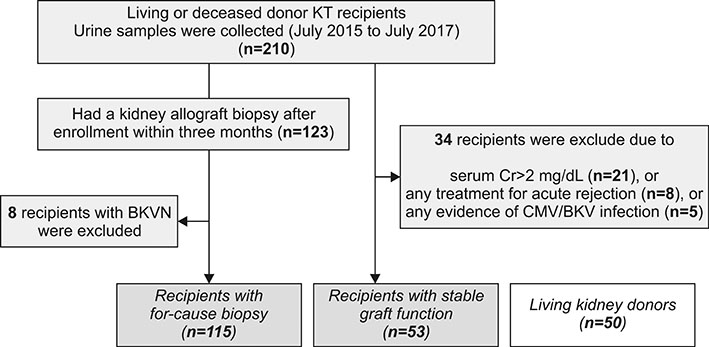
Fig. 1 Inclusion of patients (recipients with for-cause biopsy, recipients with stable graft function, and living kidney donors).
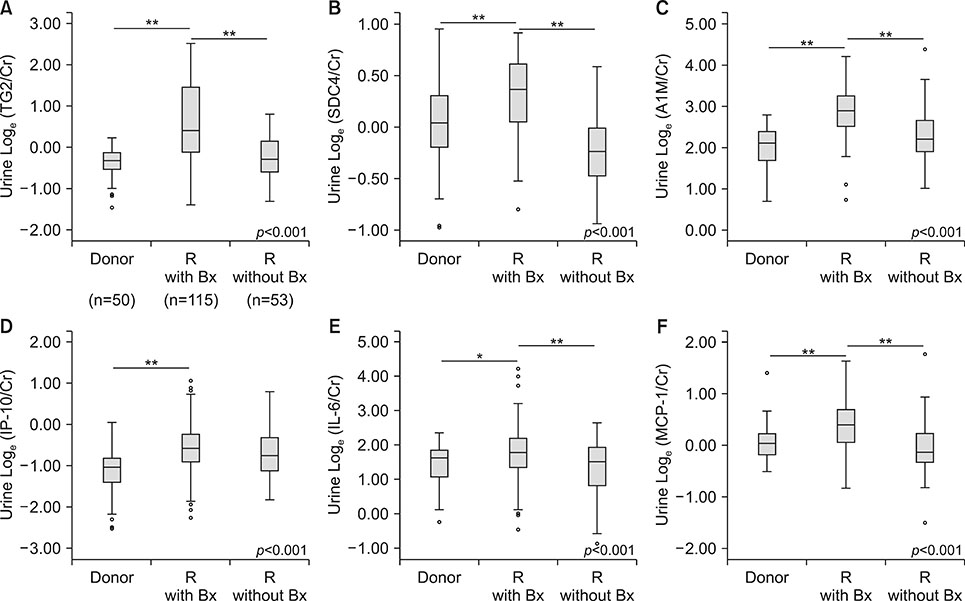
Fig. 2 Levels of urinary biomarkers in each group. Box-and-whisker plots show the loge-transformed ratios of each molecule to creatinine for TG2, SDC4, A1M, IP-10, IL-6, and MCP-1. The concentration for each biomarker as follows: TG2/Cr (ng/mg), SDC4/Cr (pg/mg), A1M/Cr (ng/mg), IP-10/Cr (pg/mg), IL-6/Cr (fg/mg), and MCP-1/Cr (pg/mg). Donor, living kidney donors; R with Bx, recipients with for-cause biopsy; R without Bx, recipients with stable graft function, *p<0.05, **p<0.001.
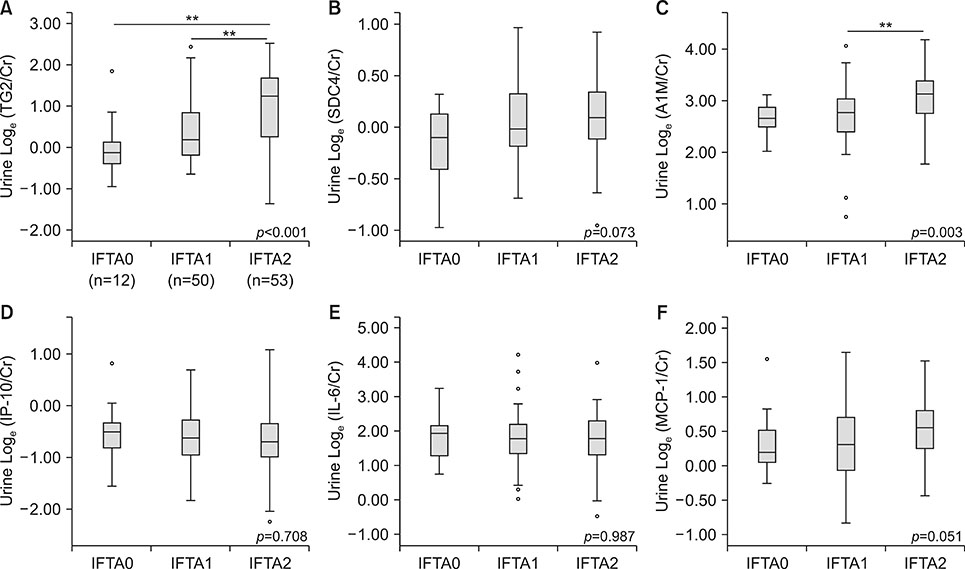
Fig. 3 Levels of urinary biomarkers according to severity of IFTA scores. Box-and-whisker plots show the loge-transformed ratios of each molecule to creatinine for TG2, SDC4, A1M, IP-10, IL-6, and MCP-1. The concentration for each biomarker as follows: TG2/Cr (ng/mg), SDC4/Cr (pg/mg), A1M/Cr (ng/mg), IP-10/Cr (pg/mg), IL-6/Cr (fg/mg), and MCP-1/Cr (pg/mg). IFTA, interstitial fibrosis and tubular atrophy; IFTA 0, minimal IFTA; IFTA 1, mild IFTA; IFTA 2, moderate to severe IFTA, **p<0.001.
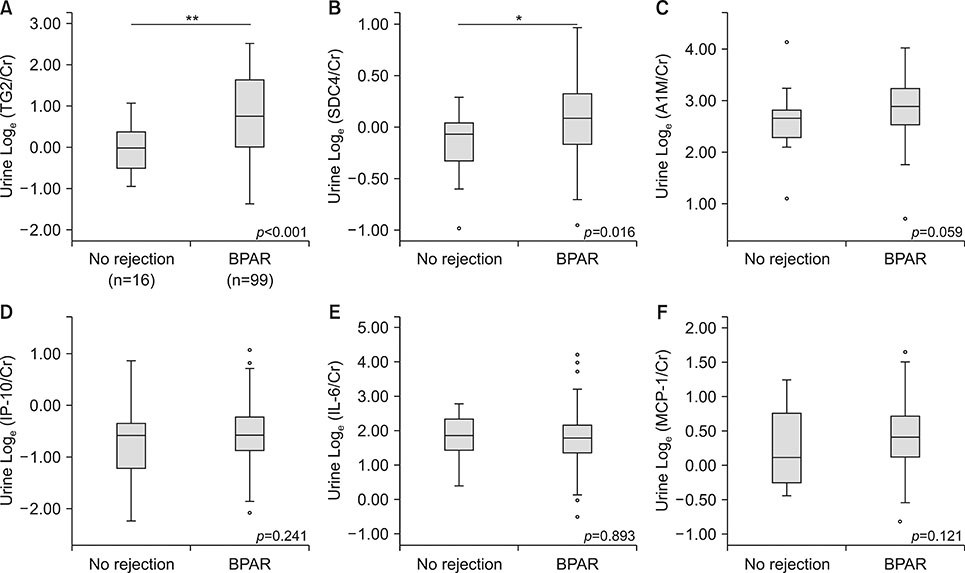
Fig. 4 Levels of urinary biomarkers according to the presence of BPAR. Box-and-whisker plots show the loge-transformed ratios of each molecule to creatinine for TG2, SDC4, A1M, IP-10, IL-6, and MCP-1. The concentration for each biomarker as follows: TG2/Cr (ng/mg), SDC4/Cr (pg/mg), A1M/Cr (ng/mg), IP-10/Cr (pg/mg), IL-6/Cr (fg/mg), and MCP-1/Cr (pg/mg). BPAR, Biopsy-proven acute rejection, *p<0.05, **p<0.001.
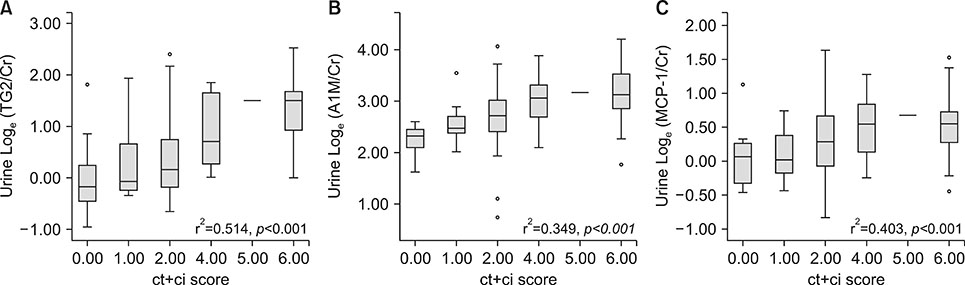
Fig. 5 Correlation analysis of ct+ci scores with urinary TG2, A1M, and MCP-1. Box-and-whisker plots show the loge-transformed ratios of TG2 (A), A1M (B), and MCP-1 (C) to creatinine according to ct+ci scores. The concentration for each biomarker as follows: TG2/Cr (ng/mg), A1M/Cr (ng/mg), and MCP-1/Cr (pg/mg).
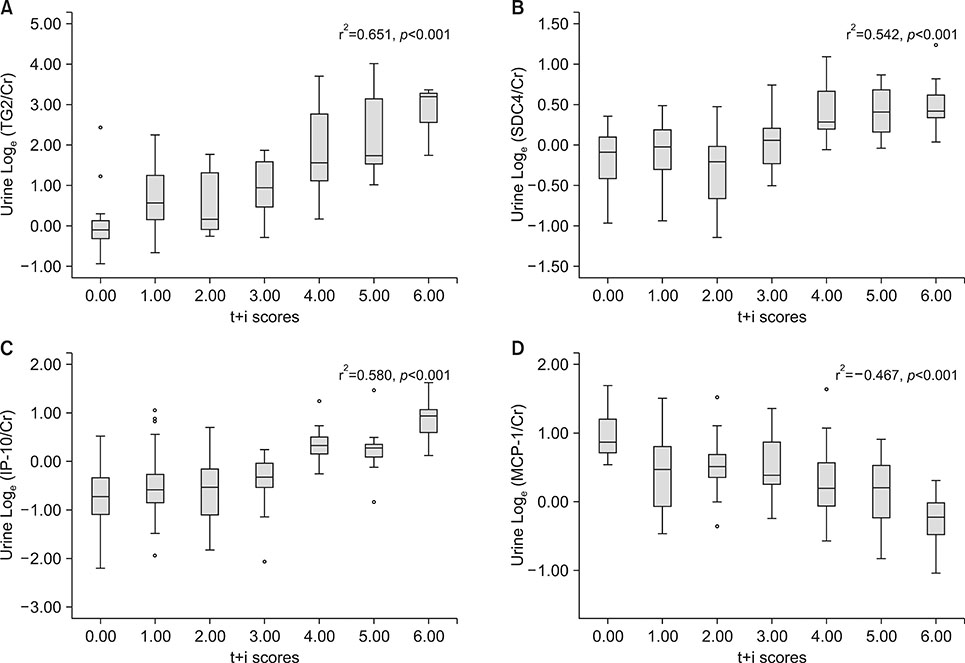
Fig. 6 Correlation analysis of ct+ci scores with urinary biomarkers. Box-and-whisker plots show the loge-transformed ratios of TG2 (A), SDC4 (B), IP-10 (C), MCP-1 (D) to creatinine according to t+i scores. The concentration for each biomarker as follows: TG2/Cr (ng/mg), SDC4/Cr (pg/mg), IP-10/Cr (pg/mg), and MCP-1/Cr (pg/mg).
Cited by 1 articles
-
Urinary transglutaminase 2 as a potent biomarker to predict interstitial fibrosis and tubular atrophy of kidney allograft during early posttransplant period in deceased donor kidney transplantation
Jee Yeon Kim, Yu-Mee Wee, Monica Young Choi, Hey Rim Jung, Ji Yoon Choi, Hyun Wook Kwon, Joo Hee Jung, Yong Mee Cho, Heounjeong Go, Minkyu Han, Young Hoon Kim, Duck Jong Han, Sung Shin
Ann Surg Treat Res. 2019;97(1):27-35. doi: 10.4174/astr.2019.97.1.27.
Reference
-
1. Naesens M, Anglicheau D. Precision transplant medicine: biomarkers to the rescue. J Am Soc Nephrol. 2018; 29:24–34.
Article2. Roedder S, Sigdel T, Salomonis N, Hsieh S, Dai H, Bestard O, et al. The kSORT assay to detect renal transplant patients at high risk for acute rejection: results of the multicenter AART study. PLoS Med. 2014; 11:e1001759.
Article3. Naesens M, Salvatierra O, Benfield M, Ettenger RB, Dharnidharka V, Harmon W, et al. Subclinical inflammation and chronic renal allograft injury in a randomized trial on steroid avoidance in pediatric kidney transplantation. Am J Transplant. 2012; 12:2730–2743.
Article4. Furness PN, Taub N. International variation in the interpretation of renal transplant biopsies: report of the CERTPAP Project. Kidney Int. 2001; 60:1998–2012.5. Haas M, Sis B, Racusen LC, Solez K, Glotz D, Colvin RB, et al. Banff 2013 meeting report: inclusion of c4d-negative antibody-mediated rejection and antibody-associated arterial lesions. Am J Transplant. 2014; 14:272–283.
Article6. Salvadori M, Tsalouchos A. Biomarkers in renal transplantation: an updated review. World J Transplant. 2017; 7:161–178.
Article7. Naesens M, Khatri P, Li L, Sigdel TK, Vitalone MJ, Chen R, et al. Progressive histological damage in renal allografts is associated with expression of innate and adaptive immunity genes. Kidney Int. 2011; 80:1364–1376.
Article8. Mas VR, Mueller TF, Archer KJ, Maluf DG. Identifying biomarkers as diagnostic tools in kidney transplantation. Expert Rev Mol Diagn. 2011; 11:183–196.
Article9. Lo DJ, Kaplan B, Kirk AD. Biomarkers for kidney transplant rejection. Nat Rev Nephrol. 2014; 10:215–225.
Article10. Fehr T, Cohen CD. Predicting an allograft's fate. Kidney Int. 2011; 80:1254–1255.
Article11. Scarpellini A, Huang L, Burhan I, Schroeder N, Funck M, Johnson TS, et al. Syndecan-4 knockout leads to reduced extracellular transglutaminase-2 and protects against tubulointerstitial fibrosis. J Am Soc Nephrol. 2014; 25:1013–1027.
Article12. Park M, Katz R, Shlipak MG, Weiner D, Tracy R, Jotwani V, et al. Urinary markers of fibrosis and risk of cardiovascular events and death in kidney transplant recipients: the FAVORIT Trial. Am J Transplant. 2017; 17:2640–2649.13. Suthanthiran M, Schwartz JE, Ding R, Abecassis M, Dadhania D, Samstein B, et al. Urinary-cell mRNA profile and acute cellular rejection in kidney allografts. N Engl J Med. 2013; 369:20–31.
Article14. Anglicheau D, Naesens M, Essig M, Gwinner W, Marquet P. Establishing biomarkers in transplant medicine: a critical review of current approaches. Transplantation. 2016; 100:2024–2038.15. Zhou H, Yuen PS, Pisitkun T, Gonzales PA, Yasuda H, Dear JW, et al. Collection, storage, preservation, and normalization of human urinary exosomes for biomarker discovery. Kidney Int. 2006; 69:1471–1476.
Article16. Price JW. Creatinine normalization of workplace urine drug tests: does it make a difference? J Addict Med. 2013; 7:129–132.17. Hricik DE, Nickerson P, Formica RN, Poggio ED, Rush D, Newell KA, et al. Multicenter validation of urinary CXCL9 as a risk-stratifying biomarker for kidney transplant injury. Am J Transplant. 2013; 13:2634–2644.
Article18. Ho J, Rush DN, Krokhin O, Antonovici M, Gao A, Bestland J, et al. Elevated urinary matrix metalloproteinase-7 detects underlying renal allograft inflammation and injury. Transplantation. 2016; 100:648–654.
Article19. Zhou D, Tian Y, Sun L, Zhou L, Xiao L, Tan RJ, et al. Matrix metalloproteinase-7 is a urinary biomarker and pathogenic mediator of kidney fibrosis. J Am Soc Nephrol. 2017; 28:598–611.
Article20. Jones RA, Kotsakis P, Johnson TS, Chau DY, Ali S, Melino G, et al. Matrix changes induced by transglutaminase 2 lead to inhibition of angiogenesis and tumor growth. Cell Death Differ. 2006; 13:1442–1453.
Article21. Melino G, Annicchiarico-Petruzzelli M, Piredda L, Candi E, Gentile V, Davies PJ, et al. Tissue transglutaminase and apoptosis: sense and antisense transfection studies with human neuroblastoma cells. Mol Cell Biol. 1994; 14:6584–6596.
Article22. Balajthy Z, Csomós K, Vámosi G, Szántó A, Lanotte M, Fésüs L. Tissue-transglutaminase contributes to neutrophil granulocyte differentiation and functions. Blood. 2006; 108:2045–2054.
Article23. Haroon ZA, Hettasch JM, Lai TS, Dewhirst MW, Greenberg CS. Tissue transglutaminase is expressed, active, and directly involved in rat dermal wound healing and angiogenesis. FASEB J. 1999; 13:1787–1795.24. Stephens P, Grenard P, Aeschlimann P, Langley M, Blain E, Errington R, et al. Crosslinking and G-protein functions of transglutaminase 2 contribute differentially to fibroblast wound healing responses. J Cell Sci. 2004; 117:3389–3403.25. Shin S, Cho YP, Jun H, Park H, Hong HN, Kwon TW. Transglutaminase type 2 in human abdominal aortic aneurysm is a potential factor in the stabilization of extracellular matrix. J Vasc Surg. 2013; 57:1362–1370.26. Weber MH, Verwiebe R. Alpha 1-microglobulin (protein HC): features of a promising indicator of proximal tubular dysfunction. Eur J Clin Chem Clin Biochem. 1992; 30:683–691.27. Amer H, Lieske JC, Rule AD, Kremers WK, Larson TS, Franco Palacios CR, et al. Urine high and low molecular weight proteins one-year post-kidney transplant: relationship to histology and graft survival. Am J Transplant. 2013; 13:676–684.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Urinary transglutaminase 2 as a potent biomarker to predict interstitial fibrosis and tubular atrophy of kidney allograft during early posttransplant period in deceased donor kidney transplantation
- Comparison between Osteopontin Expression and Renal Function in Spontaneous Renal Failure Model
- Medullary histology may help to predict Banff scores in allograft kidneys
- Relationship of Proteinuria and Graft Survival According to the Degree of Transplant Glomerulopathy
- Multicenter, prospective observational study to identify and validate a composite of urinary exosomal biomarkers for kidney allograft tubulointerstitial fibrosis
