A case of severe mandibular retrognathism with bilateral condylar deformities treated with Le Fort I osteotomy and two advancement genioplasty procedures
- Affiliations
-
- 1Department of Orthodontics, Okayama University Hospital, Okayama, Japan. yanagita@md.okayama-u.ac.jp
- 2Department of Oral and Maxillofacial Reconstructive Surgery, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama, Japan.
- 3Department of Orthodontics and Dentofacial Orthopedics, Graduate School of Dentistry, Osaka University, Osaka, Japan.
- 4Department of Orthodontics, Okayama University Graduate School of Medicine, Dentistry and Pharmaceutical Sciences, Okayama, Japan.
- KMID: 2426684
- DOI: http://doi.org/10.4041/kjod.2016.46.6.395
Abstract
- We report a case involving a young female patient with severe mandibular retrognathism accompanied by mandibular condylar deformity that was effectively treated with Le Fort I osteotomy and two genioplasty procedures. At 9 years and 9 months of age, she was diagnosed with Angle Class III malocclusion, a skeletal Class II jaw relationship, an anterior crossbite, congenital absence of some teeth, and a left-sided cleft lip and palate. Although the anterior crossbite and narrow maxillary arch were corrected by interceptive orthodontic treatment, severe mandibular hypogrowth resulted in unexpectedly severe mandibular retrognathism after growth completion. Moreover, bilateral condylar deformities were observed, and we suspected progressive condylar resorption (PCR). There was a high risk of further condylar resorption with mandibular advancement surgery; therefore, Le Fort I osteotomy with two genioplasty procedures was performed to achieve counterclockwise rotation of the mandible and avoid ingravescence of the condylar deformities. The total duration of active treatment was 42 months. The maxilla was impacted by 7.0 mm and 5.0 mm in the incisor and molar regions, respectively, while the pogonion was advanced by 18.0 mm. This significantly resolved both skeletal disharmony and malocclusion. Furthermore, the hyoid bone was advanced, the pharyngeal airway space was increased, and the morphology of the mandibular condyle was maintained. At the 30-month follow-up examination, the patient exhibited a satisfactory facial profile. The findings from our case suggest that severe mandibular retrognathism with condylar deformities can be effectively treated without surgical mandibular advancement, thus decreasing the risk of PCR.
MeSH Terms
Figure
-

Figure 1 Initial facial and intraoral photographs of our patient who was diagnosed with Angle Class III malocclusion, a skeletal Class II jaw relationship, an anterior crossbite, congenital absence of some teeth, and a left-sided cleft lip and palate at 9 years and 9 months of age.
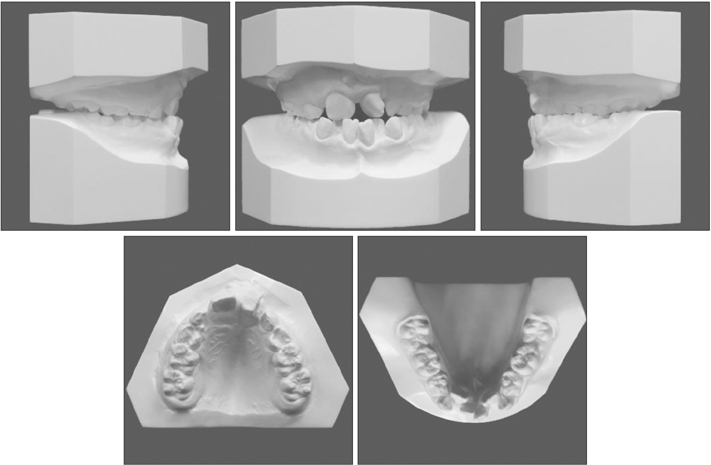
Figure 2 Initial dental casts.
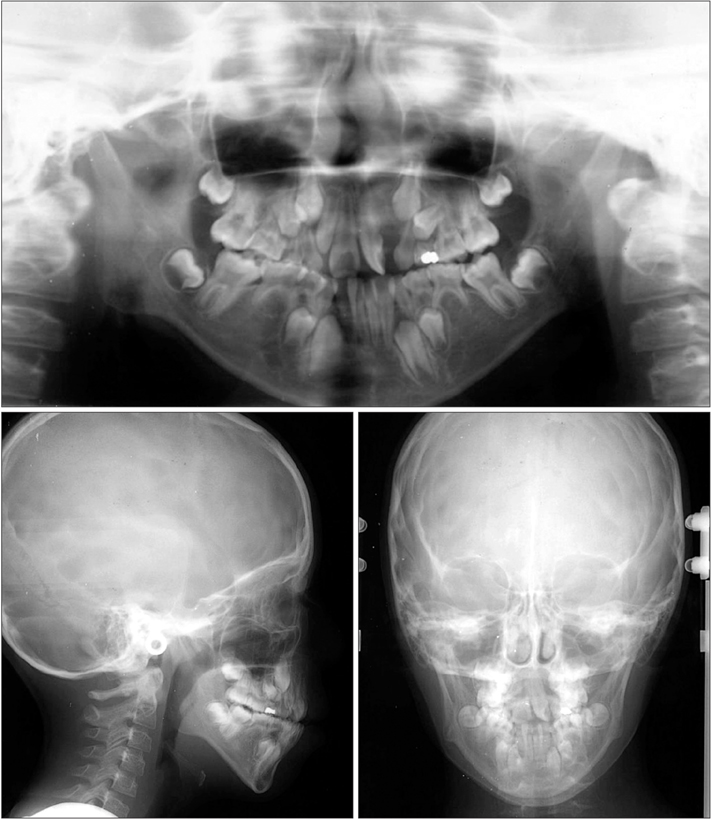
Figure 3 Initial panoramic and cephalometric radiographs.
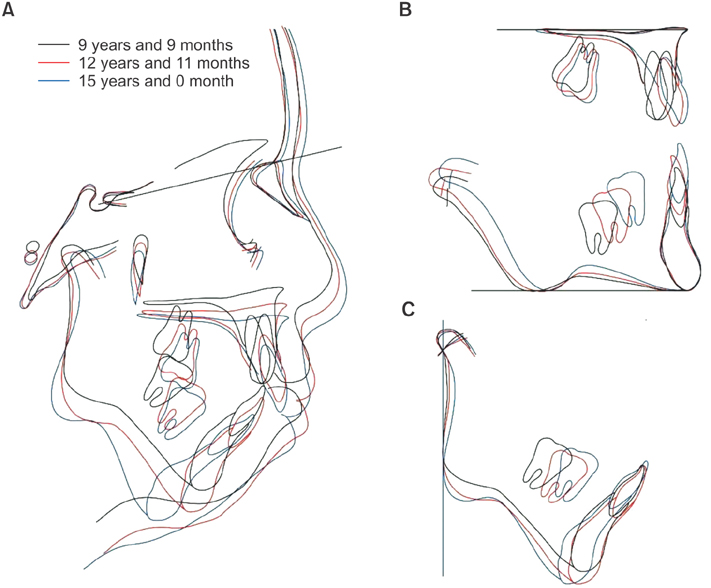
Figure 4 Superimposition of cephalometric tracings obtained before, during, and after the first phase of interceptive orthodontic treatment. A, Superimposition on the sella– nasion plane at the sella. B, Superimposition on the palatal plane at the anterior nasal spine (ANS) and the mandibular plane at the menton. C, Superimposition on the ramus plane at the articulare.

Figure 5 Facial and intraoral photographs obtained before the second phase of treatment for our patient who exhibited severe mandibular retrognathism with bilateral condylar deformities after growth completion.
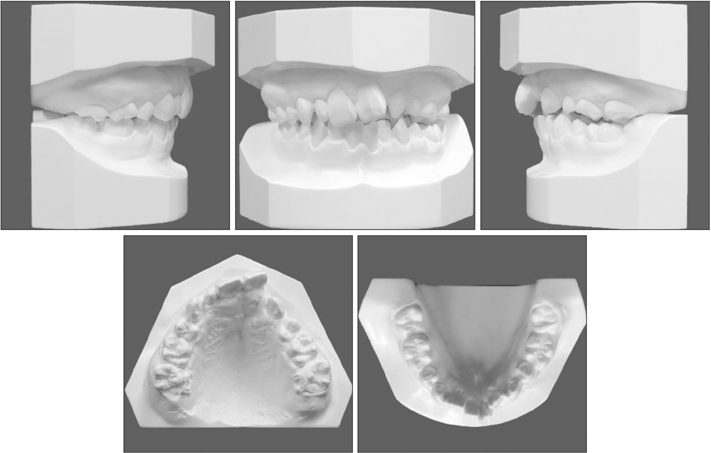
Figure 6 Dental casts fabricated before the second phase of treatment.
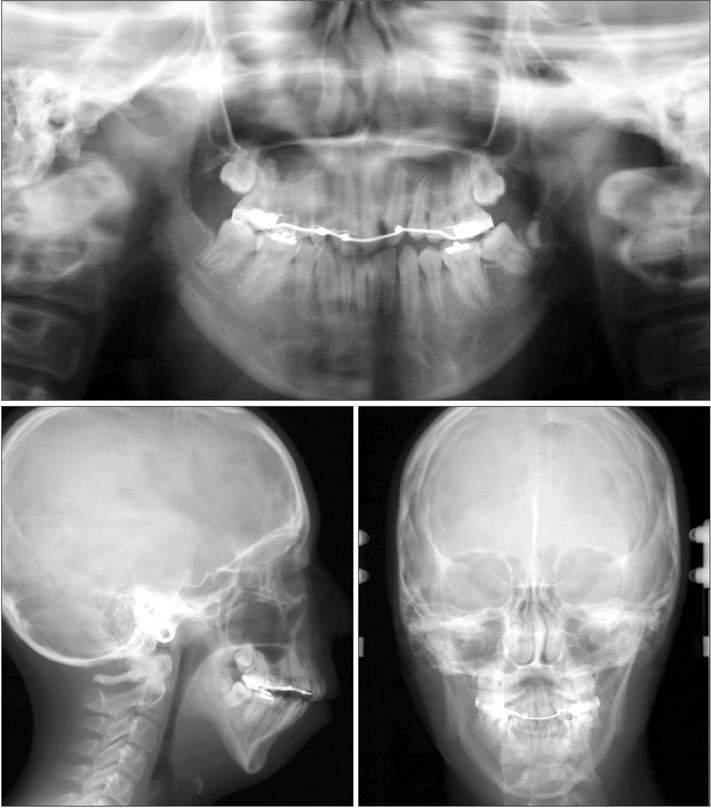
Figure 7 Panoramic and cephalometric radiographs obtained before the second phase of treatment.
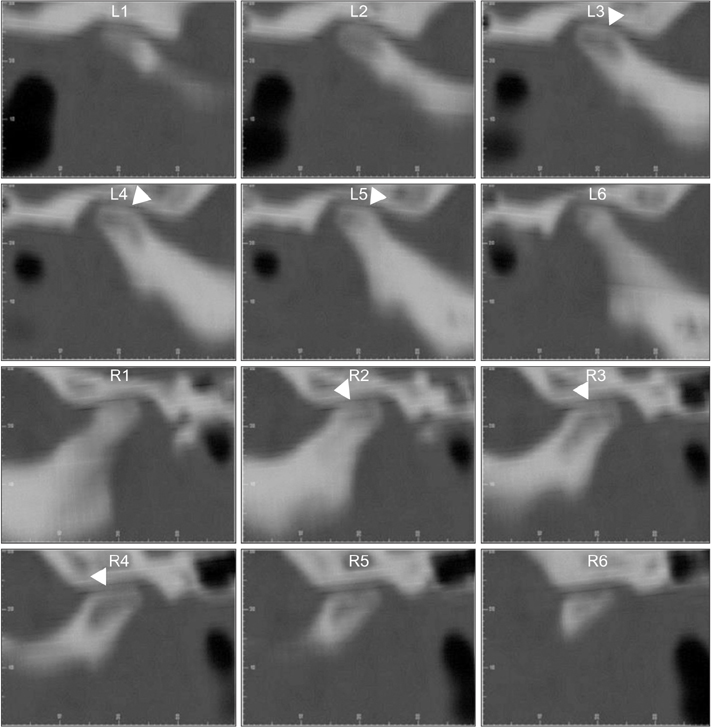
Figure 8 Computed tomography images of the bilateral condyles for our patient with bilateral condylar deformities after growth completion. The arrowheads show bone surface absorption.

Figure 9 Facial and intraoral photographs obtained after Le Fort I osteotomy with two advancement genioplasty procedures followed by fixed orthodontic treatment.
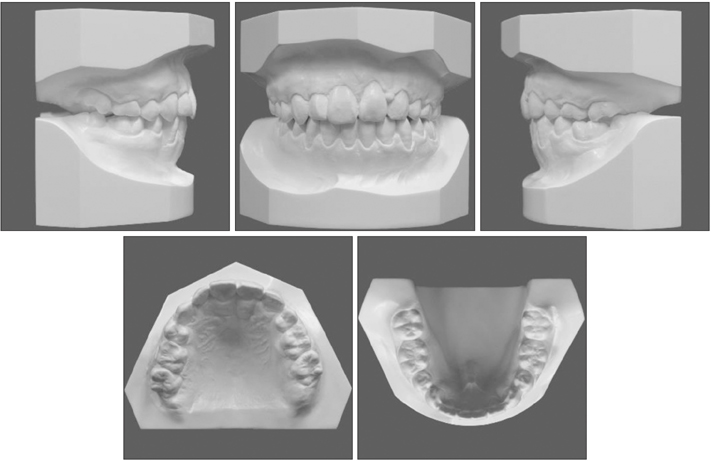
Figure 10 Dental casts fabricated after treatment.
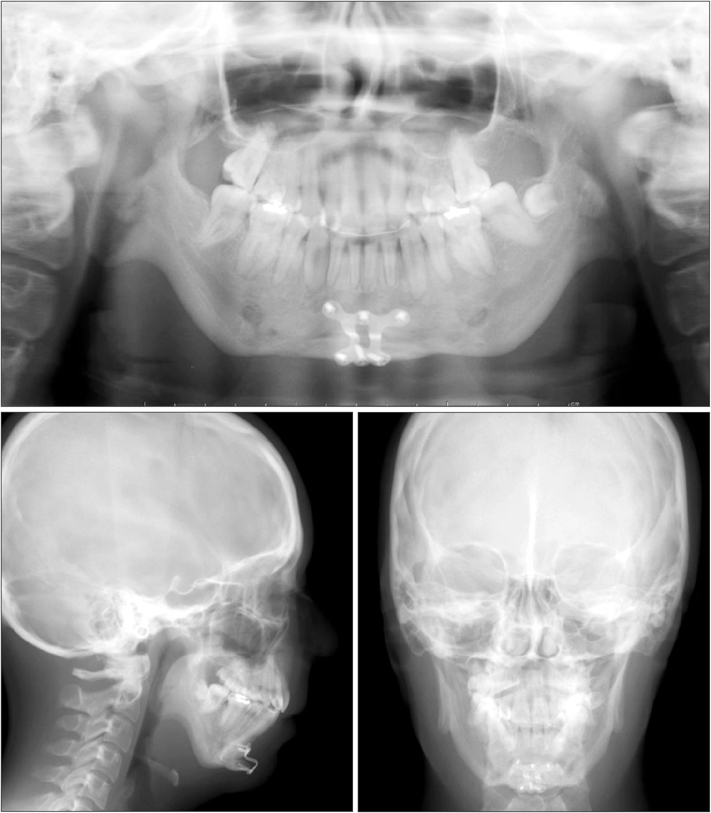
Figure 11 Panoramic and cephalometric radiographs obtained after treatment.
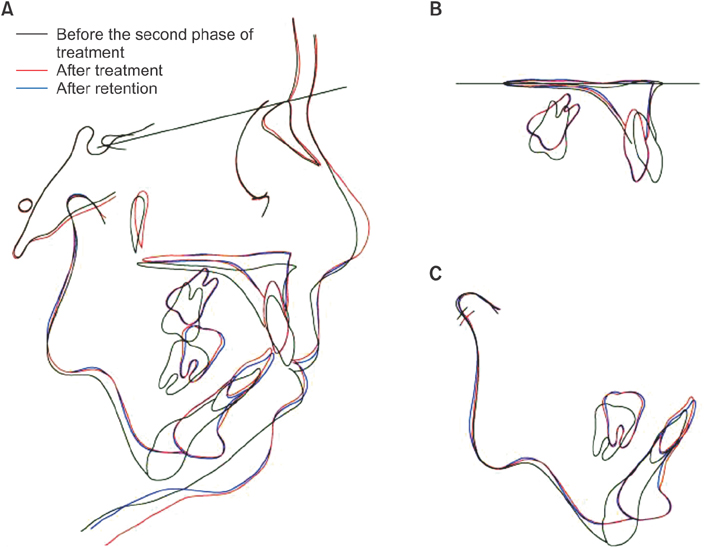
Figure 12 Superimposition of cephalometric tracings obtained before the second phase of treatment and after Le Fort I osteotomy with two advancement genioplasty procedures followed by fixed orthodontic treatment and after retention. A, Superimposition on the sellanasion plane at the sella. B, Super impo s i t ion on the palatal plane at the posterior nasal spine (PNS). C, Superimposition at the gonion.
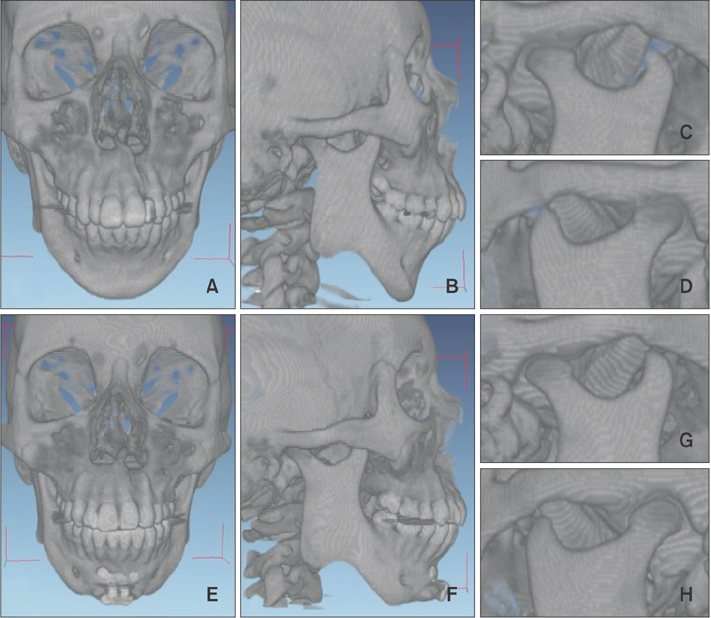
Figure 13 Computed tomography reconstructions obtained before (A–D) and after (E–F) Le Fort I osteotomy with two advancement genioplasty procedures followed by fixed orthodontic treatment and retention for our patient who exhibited severe mandibular retrognathism with bilateral condylar deformities after growth completion.

Figure 14 Assessment of the airway space after treatment. A, Superimposition of cephalometric tracings with the pharyngeal area (black, before treatment; red, after treatment). B, Airway volume measurements obtained using the Dolphin 3D software (Dolphin Imaging and Management Solutions, Chatsworth, CA, USA) for airway analysis.

Figure 15 Facial and intraoral photographs obtained at 30 months after treatment.
Reference
-
1. Proffit WR, Phillips C, Douvartzidis N. A comparison of outcomes of orthodontic and surgical-orthodontic treatment of Class II malocclusion in adults. Am J Orthod Dentofacial Orthop. 1992; 101:556–565.
Article2. Mihalik CA, Proffit WR, Phillips C. Long-term follow-up of Class II adults treated with orthodontic camouflage: a comparison with orthognathic surgery outcomes. Am J Orthod Dentofacial Orthop. 2003; 123:266–278.
Article3. Muto T, Yamazaki A, Takeda S. A cephalometric evaluation of the pharyngeal airway space in patients with mandibular retrognathia and prognathia, and normal subjects. Int J Oral Maxillofac Surg. 2008; 37:228–231.
Article4. Achilleos S, Krogstad O, Lyberg T. Surgical mandibular advancement and changes in uvuloglossopharyngeal morphology and head posture: a short- and long-term cephalometric study in males. Eur J Orthod. 2000; 22:367–381.
Article5. Proffit WR, Turvey TA, Phillips C. The hierarchy of stability and predictability in orthognathic surgery with rigid fixation: an update and extension. Head Face Med. 2007; 3:21.
Article6. Schreuder WH, Jansma J, Bierman MW, Vissink A. Distraction osteogenesis versus bilateral sagittal split osteotomy for advancement of the retrognathic mandible: a review of the literature. Int J Oral Maxillofac Surg. 2007; 36:103–110.
Article7. Baas EM, Pijpe J, de Lange J. Long term stability of mandibular advancement procedures: bilateral sagittal split osteotomy versus distraction osteogenesis. Int J Oral Maxillofac Surg. 2012; 41:137–141.
Article8. Hoppenreijs TJ, Stoelinga PJ, Grace KL, Robben CM. Long-term evaluation of patients with progressive condylar resorption following orthognathic surgery. Int J Oral Maxillofac Surg. 1999; 28:411–418.
Article9. Arnett GW, Milam SB, Gottesman L. Progressive mandibular retrusion-idiopathic condylar resorption. Part II. Am J Orthod Dentofacial Orthop. 1996; 110:117–127.
Article10. Cutbirth M, Van Sickels JE, Thrash WJ. Condylar resorption after bicortical screw fixation of mandibular advancement. J Oral Maxillofac Surg. 1998; 56:178–182. discussion 183.
Article11. Kobayashi T, Izumi N, Kojima T, Sakagami N, Saito I, Saito C. Progressive condylar resorption after mandibular advancement. Br J Oral Maxillofac Surg. 2012; 50:176–180.
Article12. Wada K, Matsushita K, Shimazaki S, Miwa Y, Hasuike Y, Susami R. An evaluation of a new case analysis of a lateral cephalometric roentgenogram. J Kanazawa Med Univ. 1981; 6:60–70.13. van Strijen PJ, Breuning KH, Becking AG, Tuinzing DB. Condylar resorption following distraction osteogenesis: a case report. J Oral Maxillofac Surg. 2001; 59:1104–1107. discussion 1107-8.
Article14. Wolford LM, Cardenas L. Idiopathic condylar resorption: diagnosis, treatment protocol, and outcomes. Am J Orthod Dentofacial Orthop. 1999; 116:667–677.
Article15. Hoppenreijs TJ, Freihofer HP, Stoelinga PJ, Tuinzing DB, van't Hof MA. Condylar remodelling and resorption after Le Fort I and bimaxillary osteotomies in patients with anterior open bite. A clinical and radiological study. Int J Oral Maxillofac Surg. 1998; 27:81–91.
Article16. Hayes RJ, Sarver DM, Jacobson A. The quantification of soft tissue cervicomental changes after mandibular advancement surgery. Am J Orthod Dentofacial Orthop. 1994; 105:383–391.
Article17. Kezirian EJ, Goldberg AN. Hypopharyngeal surgery in obstructive sleep apnea: an evidence-based medicine review. Arch Otolaryngol Head Neck Surg. 2006; 132:206–213.18. Hendler B, Silverstein K, Giannakopoulos H, Costello BJ. Mortised genioplasty in the treatment of obstructive sleep apnea: an historical perspective and modification of design. Sleep Breath. 2001; 5:173–180.
Article19. Nagler RM, Laufer D. Genioglossal advancement--a simple surgical procedure for sleep apnea. Case report and literature review. Eur Surg Res. 2002; 34:373–377.
Article20. Teittinen M, Tuovinen V, Tammela L, Schätzle M, Peltomäki T. Long-term stability of anterior open bite closure corrected by surgical-orthodontic treatment. Eur J Orthod. 2012; 34:238–243.
Article21. Pagnoni M, Amodeo G, Fadda MT, Brauner E, Guarino G, Virciglio P, et al. Juvenile idiopathic/rheumatoid arthritis and orthognatic surgery without mandibular osteotomies in the remittent phase. J Craniofac Surg. 2013; 24:1940–1945.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A case report of surgical correction of mandibular prognathism with midfacial deficiency using Le Fort III osteotomy
- Comparison of Postoperative Stability between Distraction Osteogenesis and Bilateral Sagittal Split Ramus Osteotomy in Mandibular Retrognathism
- Surgical Management of Atypical Apert Syndrome Patient Using Combined Cranial and Maxillofacial Surgery
- Combined orthodontic-surgical treatment for Class III patient with midfacial deficiency and mandibular prognathism
- Le Fort I osteotomy as treatment for traumatic class III malocclusion caused by Le Fort III fracture: A case report
