Investig Clin Urol.
2016 May;57(3):184-190. 10.4111/icu.2016.57.3.184.
Risk factors for hypertensive attack during pheochromocytoma resection
- Affiliations
-
- 1Department of Urology, Dongguk University College of Medicine, Gyeongju, Korea.
- 2Department of Urology, Kyungpook National University School of Medicine, Daegu, Korea. doctork@knu.ac.kr
- KMID: 2426492
- DOI: http://doi.org/10.4111/icu.2016.57.3.184
Abstract
- PURPOSE
We aimed to retrospectively evaluate the risk factors for hypertensive attack during adrenalectomy in patients with pheochromocytoma. Despite the development of newer surgical and anesthetic techniques for the management of pheochromocytoma, intraoperative hypertensive attack continues to present a challenge.
MATERIALS AND METHODS
Data from 53 patients diagnosed with pheochromocytoma at Kyungpook National Uriversity Medical Center between January 2000 and June 2012 were retrospectively analyzed. The subjects were divided into 2 groups depending on the presence or absence of hypertensive attack at the time of surgery. Patient demographic characteristics and preoperative evaluations were assessed for their prognostic relevance with respect to hypertensive attack. A univariate analysis was conducted, and a multivariate logistic regression analysis was also performed.
RESULTS
In the univariate analysis, systolic blood pressure at presentation, preoperative hormonal status (including epinephrine, norepinephrine, vanillylmandelic acid, and metanephrine levels in a 24-hour urine sample), tumor size, and postoperative systolic blood pressure were significantly associated with the development of hypertensive attack. In the multivariate analysis, preoperative epinephrine level and tumor size were independent factors that predicted hypertensive attack. The highest odds ratio for tumor size (2.169) was obtained at a cutoff value of 4.25 cm and the highest odds ratio for preoperative epinephrine (1.020) was obtained at a cutoff value of 166.3 µg/d.
CONCLUSIONS
In this study, a large tumor size and an elevated preoperative urinary epinephrine level were risk factors for intraoperative hypertensive attack in patients with pheochromocytoma.
Keyword
MeSH Terms
-
Adrenal Gland Neoplasms/physiopathology/*surgery
Adrenalectomy/*adverse effects
Adult
Blood Pressure/physiology
Catecholamines/urine
Female
Humans
Hypertension/*etiology/physiopathology/urine
Intraoperative Complications
Male
Middle Aged
Pheochromocytoma/physiopathology/*surgery
Prognosis
ROC Curve
Retrospective Studies
Risk Factors
Figure
-
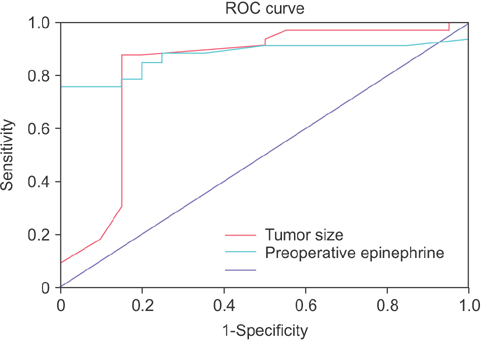
Fig. 1 Receiver operating characteristic (ROC) curve of multiple cutoff values of tumor size and preoperative epinephrine.
Reference
-
1. Lenders JW, Eisenhofer G, Mannelli M, Pacak K. Phaeochromocytoma. Lancet. 2005; 366:665–675.2. Plouin PF, Duclos JM, Soppelsa F, Boublil G, Chatellier G. Factors associated with perioperative morbidity and mortality in patients with pheochromocytoma: analysis of 165 operations at a single center. J Clin Endocrinol Metab. 2001; 86:1480–1486.3. Manger WM, Gifford RW Jr, Hoffman BB. Pheochromocytoma: a clinical and experimental overview. Curr Probl Cancer. 1985; 9:1–89.4. Lo CY, van Heerden JA, Grant CS, Soreide JA, Warner MA, Ilstrup DM. Adrenal surgery in the elderly: too risky? World J Surg. 1996; 20:368–373.5. Sutton MG, Sheps SG, Lie JT. Prevalence of clinically unsuspected pheochromocytoma. Review of a 50-year autopsy series. Mayo Clin Proc. 1981; 56:354–360.6. Apgar V, Papper EM. Pheochromocytoma. Anesthetic management during surgical treatment. AMA Arch Surg. 1951; 62:634–648.7. van Heerden JA. First encounters with pheochromocytoma. The story of Mother Joachim. Am J Surg. 1982; 144:277–279.8. van Heerden JA, Roland CF, Carney JA, Sheps SG, Grant CS. Long-term evaluation following resection of apparently benign pheochromocytoma(s)/paraganglioma(s). World J Surg. 1990; 14:325–329.9. Gagner M, Lacroix A, Bolte E. Laparoscopic adrenalectomy in Cushing's syndrome and pheochromocytoma. N Engl J Med. 1992; 327:1033.10. Smith CD, Weber CJ, Amerson JR. Laparoscopic adrenalectomy: new gold standard. World J Surg. 1999; 23:389–396.11. Duh QY, Siperstein AE, Clark OH, Schecter WP, Horn JK, Harrison MR, et al. Laparoscopic adrenalectomy. Comparison of the lateral and posterior approaches. Arch Surg. 1996; 131:870–875.12. Brunt LM, Doherty GM, Norton JA, Soper NJ, Quasebarth MA, Moley JF. Laparoscopic adrenalectomy compared to open adrenalectomy for benign adrenal neoplasms. J Am Coll Surg. 1996; 183:1–10.13. Pacak K. Preoperative management of the pheochromocytoma patient. J Clin Endocrinol Metab. 2007; 92:4069–4079.14. Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg. 2009; 250:187–196.15. Saegesser F. César Roux (1857-1934) and his times. Rev Med Suisse Romande. 1984; 104:403–464.16. Winfield HN, Hamilton BD, Bravo EL, Novick AC. Laparoscopic adrenalectomy: the preferred choice? A comparison to open adrenalectomy. J Urol. 1998; 160:325–329.17. Suzuki K, Kageyama S, Hirano Y, Ushiyama T, Rajamahanty S, Fujita K. Comparison of 3 surgical approaches to laparoscopic adrenalectomy: a nonrandomized, background matched analysis. J Urol. 2001; 166:437–443.18. Bonjer HJ, Sorm V, Berends FJ, Kazemier G, Steyerberg EW, de Herder WW, et al. Endoscopic retroperitoneal adrenalectomy: lessons learned from 111 consecutive cases. Ann Surg. 2000; 232:796–803.19. Suzuki K, Ushiyama T, Ihara H, Kageyama S, Mugiya S, Fujita K. Complications of laparoscopic adrenalectomy in 75 patients treated by the same surgeon. Eur Urol. 1999; 36:40–47.20. Zhang X, Lang B, Ouyang JZ, Fu B, Zhang J, Xu K, et al. Retroperitoneoscopic adrenalectomy without previous control of adrenal vein is feasible and safe for pheochromocytoma. Urology. 2007; 69:849–853.21. Kinney MA, Warner ME, vanHeerden JA, Horlocker TT, Young WF Jr, Schroeder DR, et al. Perianesthetic risks and outcomes of pheochromocytoma and paraganglioma resection. Anesth Analg. 2000; 91:1118–1123.22. Scholten A, Vriens MR, Cromheecke GJ, Borel Rinkes IH, Valk GD. Hemodynamic instability during resection of pheochromocytoma in MEN versus non-MEN patients. Eur J Endocrinol. 2011; 165:91–96.23. Bruynzeel H, Feelders RA, Groenland TH, van den Meiracker AH, van Eijck CH, Lange JF, et al. Risk factors for hemodynamic instability during surgery for pheochromocytoma. J Clin Endocrinol Metab. 2010; 95:678–685.24. Tauzin-Fin P, Sesay M, Gosse P, Ballanger P. Effects of perioperative alpha1 block on haemodynamic control during laparoscopic surgery for phaeochromocytoma. Br J Anaesth. 2004; 92:512–517.25. Kocak S, Aydintug S, Canakci N. Alpha blockade in preoperative preparation of patients with pheochromocytomas. Int Surg. 2002; 87:191–194.26. Yang RL, Liu DW, Long Y, Shi Y, Chai WZ, Li HZ, et al. Perioperative hemodynamics in pheochromocytoma secreting different types of catecholamine. Zhonghua Yi Xue Za Zhi. 2008; 88:816–819.27. Desmonts JM, Marty J. Anaesthetic management of patients with phaeochromocytoma. Br J Anaesth. 1984; 56:781–789.28. Guerrero MA, Schreinemakers JM, Vriens MR, Suh I, Hwang J, Shen WT, et al. Clinical spectrum of pheochromocytoma. J Am Coll Surg. 2009; 209:727–732.29. Kiernan CM, Du L, Chen X, Broome JT, Shi C, Peters MF, et al. Predictors of hemodynamic instability during surgery for pheochromocytoma. Ann Surg Oncol. 2014; 21:3865–3871.
