Miliary Tuberculosis Mimicking Brain Metastasis from Renal Cell Carcinoma
- Affiliations
-
- 1Department of Pulmonary and Critical Care Medicine, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea.
- 2Department of Neurology, Busan Paik Hospital, Inje University College of Medicine, Busan, Korea.
- 3Department of Neurology, Kangdong Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. brainyrk@gmail.com
- KMID: 2426214
- DOI: http://doi.org/10.18700/jnc.180045
Abstract
- BACKGROUND
Miliary tuberculosis (TB) can cause diagnostic confusion for clinicians because its radiological appearance can resemble that of metastatic cancer.
CASE REPORT
Here, we describe the case of a 72-yearold woman with miliary TB mimicking brain metastasis from renal cell carcinoma. The patient visited our clinic because of dysarthria and sluggish speech. A metastatic cancer such as renal cell carcinoma or brain tumor was suspected. However, the patient was diagnosed with miliary TB associated with multiple intracranial tuberculomas and a subsequent paradoxical response to anti-TB therapy.
CONCLUSION
Clinicians should be aware that miliary TB can mimic metastatic cancer even in older people, especially in TB-endemic regions.
MeSH Terms
Figure
-
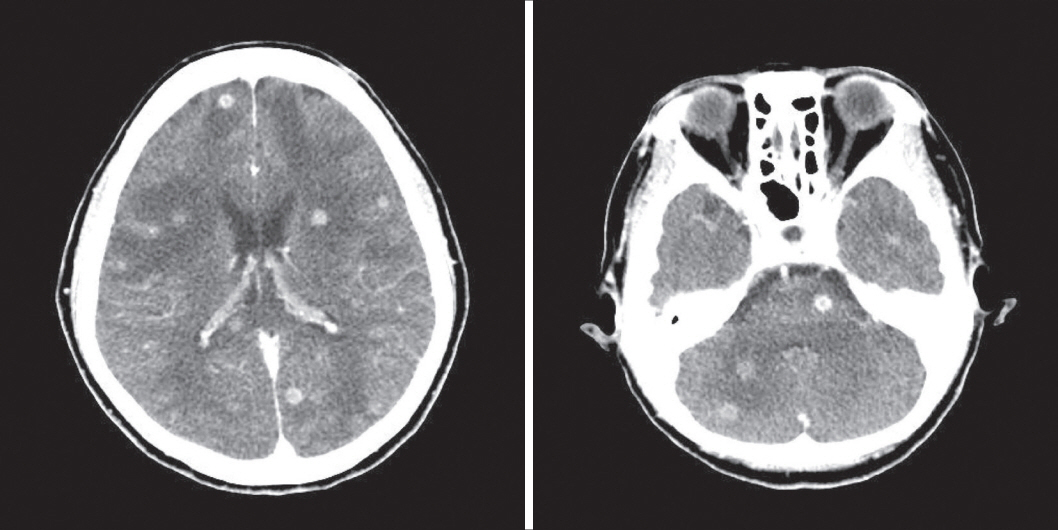
Figure 1. Axial images of contrast-enhanced computed tomography of the brain show numerous small enhancing masses with marked surrounding edema in both cerebral and cerebellar hemispheres and the brain stem.

Figure 2. Magnetic resonance imaging of the brain on admission. (A, B) T1- and T2-weighted axial images, and an image with gadolinium enhancement. Multiple ring-enhancing lesions with surrounding edema are seen in both hemispheres. (C) Diffusion-weighted images. Some abnormal restricted lesions are seen in both hemispheres.

Figure 3. (A) Chest radiograph at the time of presentation shows diffuse micronodules involving both lung fields. (B) Chest computed tomography scan in the lung window reveals uniform-sized small nodules randomly distributed throughout both lungs.
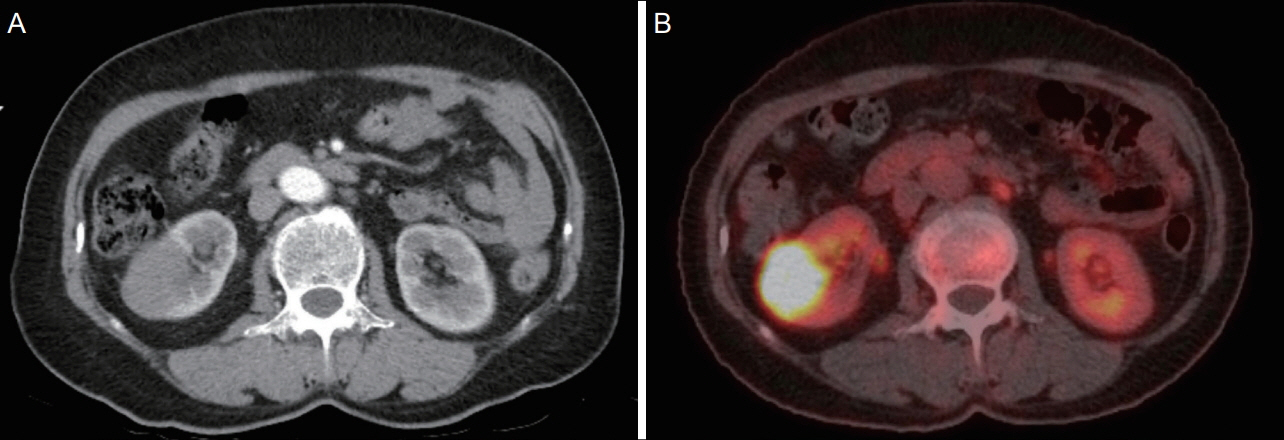
Figure 4. (A) Contrast-enhanced CT scan of the abdomen shows a 3.0×4.5 cm enhancing mass in the right lower kidney. (B) PET/CT of a fused transaxial view shows high fluorodeoxyglucose uptake (SUVmax=19.5) at the same site. CT, computed tomography; PET, positron emission tomography; SUVmax, maximum standardized uptake value.
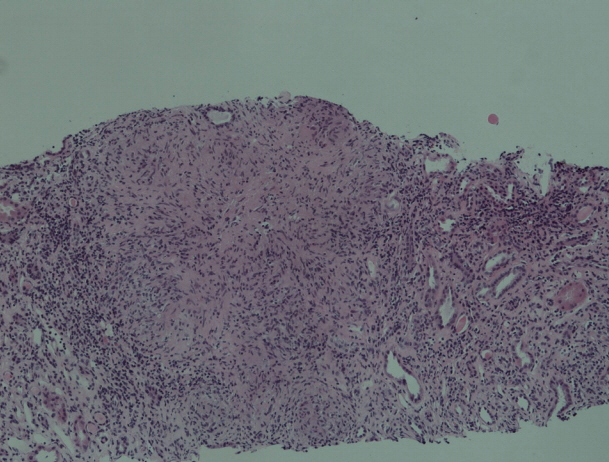
Figure 5. Percutaneous needle biopsy of the right kidney shows well-formed granulomas scattered in the interstitium of the medulla without obvious necrosis (hematoxylin and eosin staining, ×100).
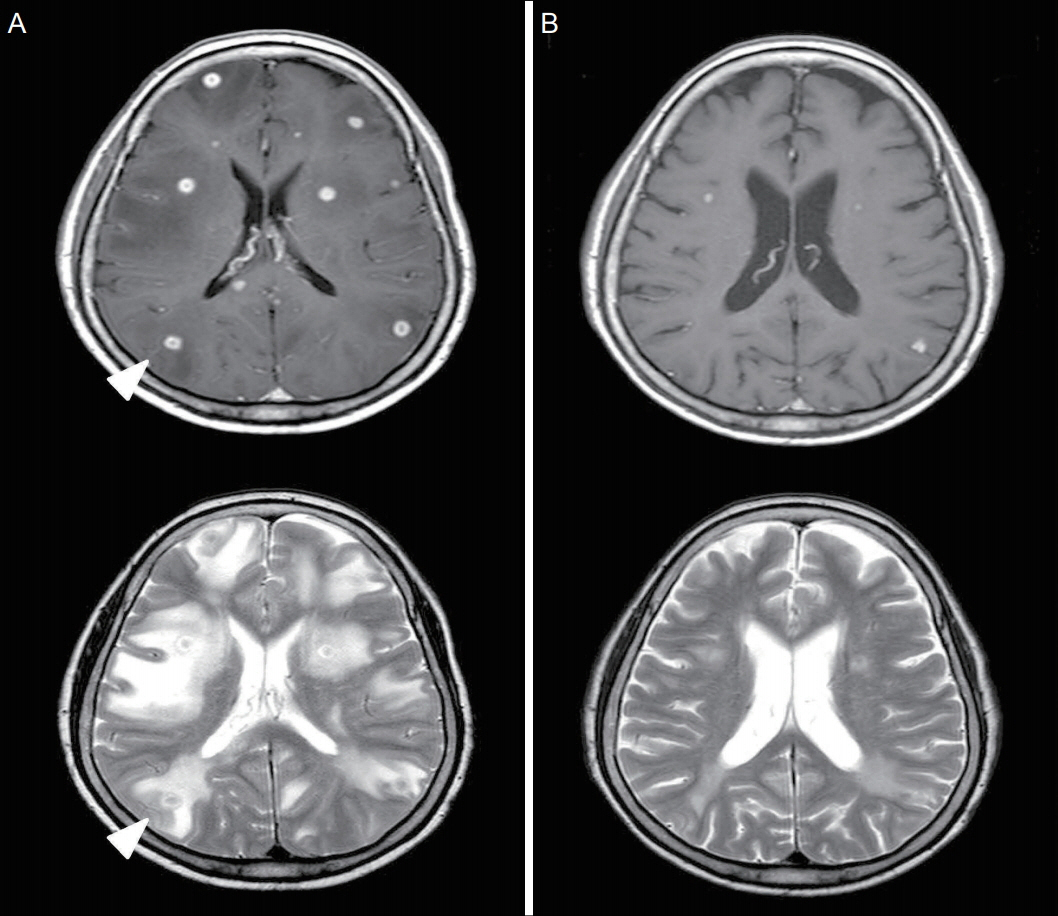
Figure 6. MRI of the brain on follow-up. (A) Follow-up brain MRI after one month of anti-tuberculosis therapy reveals no gross intervening change in the numerous small, ring-enhancing nodules. Several new lesions had developed (arrowheads). (B) Follow-up brain MRI at three months after symptom onset shows a significant decrease in the size and number of lesions and a marked amelioration of the surrounding edema. MRI, magnetic resonance imaging.
Reference
-
1. Centers for Disease Control and Prevention. Reported tuberculosis in the United States, 2012 [online]. Available at: https://www.cdc.gov/tb/. Accessed at April 5, 2018.2. Greschus S, Kuchelmeister K, Oeynhausen S, Fischer HP, Urbach H. Cerebral tuberculoma mimicking brain tumor. Clin Neuroradiol. 2014; 24:389–93.
Article3. Sharma SK, Mohan A, Sharma A, Mitra DK. Miliary tuberculosis: new insights into an old disease. Lancet Infect Dis. 2005; 5:415–30.
Article4. Ko KT, Na DJ, Han SH, Jung SS, Moon KM, Kim DJ, et al. Unusual presentation of miliary tuberculosis. Tuberc Respir Dis. 2007; 63:67–71.
Article5. Sharma SK, Mohan A, Sharma A. Challenges in the diagnosis & treatment of miliary tuberculosis. Indian J Med Res. 2012; 135:703–30.6. Burk JR, Viroslav J, Bynum LJ. Miliary tuberculosis diagnosed by fibreoptic bronchoscopy and transbronchial biopsy. Tubercle. 1978; 59:107–9.
Article7. Wasay M. Central nervous system tuberculosis and paradoxical response. South Med J. 2006; 99:331–2.
Article8. Breen RA, Smith CJ, Bettinson H, Dart S, Bannister B, Johnson MA, et al. Paradoxical reactions during tuberculosis treatment in patients with and without HIV co-infection. Thorax. 2004; 59:704–7.
Article9. Cheng VC, Yam WC, Woo PC, Lau SK, Hung IF, Wong SP, et al. Risk factors for development of paradoxical response during antituberculosis therapy in HIV-negative patients. Eur J Clin Microbiol Infect Dis. 2003; 22:597–602.
Article10. Singh AK, Malhotra HS, Garg RK, Jain A, Kumar N, Kohli N, et al. Paradoxical reaction in tuberculous meningitis: presentation, predictors and impact on prognosis. BMC Infect Dis. 2016; 16:306.
Article11. Garg RK, Sinha MK. Multiple ring-enhancing lesions of the brain. J Postgrad Med. 2010; 56:307–16.
Article12. Rock RB, Olin M, Baker CA, Molitor TW, Peterson PK. Central nervous system tuberculosis: pathogenesis and clinical aspects. Clin Microbiol Rev. 2008; 21:243–61. table of contents.
Article13. Baker CA, Cartwright CP, Williams DN, Nelson SM, Peterson PK. Early detection of central nervous system tuberculosis with the gen-probe nucleic Acid amplification assay: utility in an inner city hospital. Clin Infect Dis. 2002; 35:339–42.
Article14. Lin JJ, Harn HJ, Hsu YD, Tsao WL, Lee HS, Lee WH. Rapid diagnosis of tuberculous meningitis by polymerase chain reaction assay of cerebrospinal fluid. J Neurol. 1995; 242:147–52.
Article15. Möller-Hartmann W, Herminghaus S, Krings T, Marquardt G, Lanfermann H, Pilatus U, et al. Clinical application of proton magnetic resonance spectroscopy in the diagnosis of intracranial mass lesions. Neuroradiology. 2002; 44:371–81.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Miliary Tuberculosis and Multiple Intracranial Tuberculoma : A Case Report
- A Case of Subcutaneous Tissue Metastasis of Renal Cell Carcinoma
- A Case of Metastatic Tuberculosis Abscess Associated with Miliary Tuberculosis
- A Case of Cervical Adenocarcinoma with Pulmonary Metastasis Resembling Miliary Tuberculosis
- Comparison of High-resolution CT Findings between Miliary Metastases and Miliary Tuberculosis
