Ultrasound-Guided Intraoperative Radiofrequency Ablation and Surgical Resection for Liver Metastasis from Malignant Gastrointestinal Stromal Tumors
- Affiliations
-
- 1Department of Radiology, Asan Medical Center, Ulsan University College of Medicine, Seoul 05505, Korea. heungkyu.ko@gmail.com
- 2Department of Surgery, Asan Medical Center, Ulsan University College of Medicine, Seoul 05505, Korea.
- 3Department of Oncology, Asan Medical Center, Ulsan University College of Medicine, Seoul 05505, Korea.
- KMID: 2425109
- DOI: http://doi.org/10.3348/kjr.2018.19.1.54
Abstract
OBJECTIVE
To evaluate the effectiveness, safety, and feasibility of intraoperative radiofrequency ablation (IORFA) under ultrasound guidance for the treatment of liver metastases from gastrointestinal stromal tumors (GISTs).
MATERIALS AND METHODS
From August 2009 to February 2017, 24 patients with liver metastases of GISTs underwent IORFA, 14 underwent concurrent IORFA and primary GIST resection, and 10 underwent IORFA to treat hepatic recurrence after previous primary GIST resection. Seventy-six hepatic metastases were treated, of which 47 were surgically resected and 29 underwent IORFA. All included patients received imatinib therapy as standard treatment before and after IORFA or surgical resection. A retrospective medical record review was conducted, and follow-up data were collected. Technical success and effectiveness, overall and GIST-specific survival, and complications were assessed.
RESULTS
The mean follow-up duration was 50.7 ± 34.7 months. The technical success rate of IORFA was 100%. New metastases developed in three of the 24 patients (12.5%) following a complete response 16, 51, and 95 months after IORFA, respectively. The cumulative one-, three-, and five-year overall survival rates were 100, 94.4, and 87.7%, respectively. The one-, three-, and five-year GIST-related survival rates were 100, 94.4, and 94.4%, respectively. Two major complications (biliary stricture and hepatic abscess) were observed.
CONCLUSION
IORFA appears to be a feasible and safe treatment option for liver metastasis in patients with primary GISTs. In addition, IORFA and surgical resection may be complementary, helping to obtain complete response in cases of otherwise inoperable liver metastases secondary to GISTs.
MeSH Terms
Figure
-
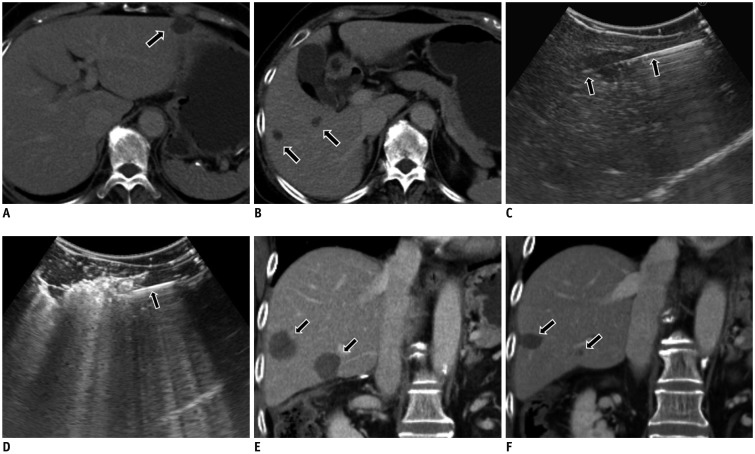
Fig. 1 71-year-old female patient (No. 13) presented with three liver metastases.A. Metastatic tumor in left lateral segment (arrow on axial CT) was surgically resected. B. Two tumors (arrows) in right lobe were ablated because of suspected hepatic failure after extensive hepatectomy. C. Radiofrequency electrode (arrows) was placed in hepatic tumor under intraoperative ultrasound guidance. D. Echogenic bubble was noted at tip of electrode (arrow) during ablation. E. Coronal CT image obtained seven days after IORFA shows two ablated zones (arrows) with complete coverage. F. Coronal CT image obtained 13 months after IORFA shows no evidence of local tumor progression. Ablation zones (arrows) indicate considerable decrease in size. CT = computed tomography, IORFA = intraoperative radiofrequency ablation
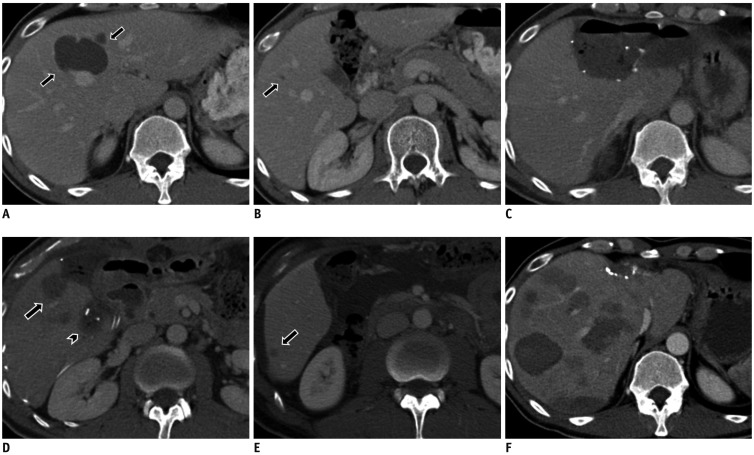
Fig. 2 38-year-old male (Patient 7) presented with five liver metastases.A. Metastatic tumors in segment 4 (arrows, axial CT) were surgically resected with sub-capsular metastatic tumors. B. Tumor (arrow) in right lobe could not be removed surgically because of risk of hepatic failure after extensive hepatectomy. C. Left lobectomy was performed to remove bulk of main metastases. D. IORFA (arrow) was performed for tumor located deep in right lobe. Partial hepatectomy (arrowhead) for sub-capsular tumor is visible. E. Axial CT image obtained five months after IORFA shows single recurrence (arrow) in right lobe. F. Axial CT image obtained 10 months after IORFA shows progression of multiple tumors and recurrence in remaining liver.
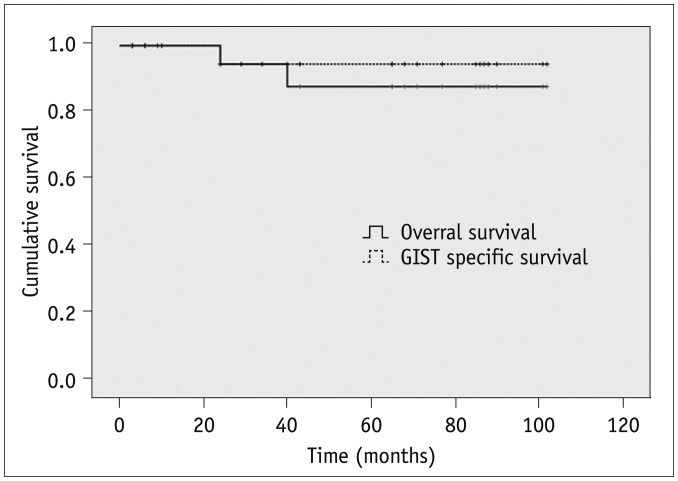
Fig. 3 Survival curves for overall and GIST-specific survival after IORFA.Five-year overall and GIST-specific survival rate was 87.7% and 94.4%, respectively. GIST = gastrointestinal stromal tumor
Reference
-
1. Correa-Cote J, Morales-Uribe C, Sanabria A. Laparoscopic management of gastric gastrointestinal stromal tumors. World J Gastrointest Endosc. 2014; 6:296–303. PMID: 25031788.
Article2. Yamanaka T, Takaki H, Nakatsuka A, Uraki J, Fujimori M, Hasegawa T, et al. Radiofrequency ablation for liver metastasis from gastrointestinal stromal tumor. J Vasc Interv Radiol. 2013; 24:341–346. PMID: 23352855.
Article3. Jung JH, Won HJ, Shin YM, Kim PN. Safety and efficacy of radiofrequency ablation for hepatic metastases from gastrointestinal stromal tumor. J Vasc Interv Radiol. 2015; 26:1797–1802. PMID: 26603498.
Article4. Joensuu H, Roberts PJ, Sarlomo-Rikala M, Andersson LC, Tervahartiala P, Tuveson D, et al. Effect of the tyrosine kinase inhibitor STI571 in a patient with a metastatic gastrointestinal stromal tumor. N Engl J Med. 2001; 344:1052–1056. PMID: 11287975.
Article5. Park SJ, Ryu MH, Ryoo BY, Park YS, Sohn BS, Kim HJ, et al. The role of surgical resection following imatinib treatment in patients with recurrent or metastatic gastrointestinal stromal tumors: results of propensity score analyses. Ann Surg Oncol. 2014; 21:4211–4217. PMID: 24980089.
Article6. Verweij J, Casali PG, Zalcberg J, LeCesne A, Reichardt P, Blay JY, et al. Progression-free survival in gastrointestinal stromal tumours with high-dose imatinib: randomised trial. Lancet. 2004; 364:1127–1134. PMID: 15451219.
Article7. An HJ, Ryu MH, Ryoo BY, Sohn BS, Kim KH, Oh ST, et al. The effects of surgical cytoreduction prior to imatinib therapy on the prognosis of patients with advanced GIST. Ann Surg Oncol. 2013; 20:4212–4218. PMID: 24052319.
Article8. Kang YK, Kang HJ, Kim KM, Sohn T, Choi D, Ryu MH, et al. Clinical practice guideline for accurate diagnosis and effective treatment of gastrointestinal stromal tumor in Korea. Cancer Res Treat. 2012; 44:85–96. PMID: 22802746.
Article9. ESMO/European Sarcoma Network Working Group. Soft tissue and visceral sarcomas: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann Oncol. 2012; 23(Suppl 7):vii92–vii99. PMID: 22997462.10. Tepel J, Hinz S, Klomp HJ, Kapischke M, Kremer B. Intraoperative radiofrequency ablation (RFA) for irresectable liver malignancies. Eur J Surg Oncol. 2004; 30:551–555. PMID: 15135485.
Article11. Eisele RM, Zhukowa J, Chopra S, Schmidt SC, Neumann U, Pratschke J, et al. Results of liver resection in combination with radiofrequency ablation for hepatic malignancies. Eur J Surg Oncol. 2010; 36:269–274. PMID: 19726155.
Article12. Park SI, Kim IJ, Lee SJ, Shin MW, Shin WS, Chung YE, et al. Angled cool-tip electrode for radiofrequency ablation of small superficial subcapsular tumors in the liver: a feasibility study. Korean J Radiol. 2016; 17:742–749. PMID: 27587963.
Article13. Wang X, Hu Y, Ren M, Lu X, Lu G, He S. Efficacy and safety of radiofrequency ablation combined with transcatheter arterial chemoembolization for hepatocellular carcinomas compared with radiofrequency ablation alone: a time-to-event meta-analysis. Korean J Radiol. 2016; 17:93–102. PMID: 26798221.
Article14. Hakimé A, Le Cesne A, Deschamps F, Farouil G, Boudabous S, Aupérin A, et al. A role for adjuvant RFA in managing hepatic metastases from gastrointestinal stromal tumors (GIST) after treatment with targeted systemic therapy using kinase inhibitors. Cardiovasc Intervent Radiol. 2014; 37:132–139. PMID: 23589213.
Article15. Pawlik TM, Vauthey JN, Abdalla EK, Pollock RE, Ellis LM, Curley SA. Results of a single-center experience with resection and ablation for sarcoma metastatic to the liver. Arch Surg. 2006; 141:537–543. discussion 543-544. PMID: 16785353.
Article16. Ishikawa A, Teratani T, Ono S, Ochiai T, Kakinoki N, Kishimoto Y, et al. [A case of gastrointestinal stromal tumor with liver and bone metastases effectively treated with radiofrequency ablation and imatinib mesylate]. Nihon Shokakibyo Gakkai Zasshi. 2006; 103:1274–1279. PMID: 17085910.17. Jones RL, McCall J, Adam A, O'Donnell D, Ashley S, Al-Muderis O, et al. Radiofrequency ablation is a feasible therapeutic option in the multi modality management of sarcoma. Eur J Surg Oncol. 2010; 36:477–482. PMID: 20060679.
Article18. Strasberg SM. Nomenclature of hepatic anatomy and resections: a review of the Brisbane 2000 system. J Hepatobiliary Pancreat Surg. 2005; 12:351–355. PMID: 16258801.
Article19. Ahmed M, Solbiati L, Brace CL, Breen DJ, Callstrom MR, Charboneau JW, et al. Image-guided tumor ablation: standardization of terminology and reporting criteria--a 10-year update. J Vasc Interv Radiol. 2014; 25:1691–1705.e4. PMID: 25442132.
Article20. Vassos N, Agaimy A, Hohenberger W, Croner RS. Management of liver metastases of gastrointestinal stromal tumors (GIST). Ann Hepatol. 2015; 14:531–539. PMID: 26019040.
Article21. Ye YJ, Gao ZD, Poston GJ, Wang S. Diagnosis and multidisciplinary management of hepatic metastases from gastrointestinal stromal tumour (GIST). Eur J Surg Oncol. 2009; 35:787–792. PMID: 19185444.
Article22. Sato T, Ohyama S, Kokudo N, Suenaga M, Yamamoto J, Yamaguchi T, et al. The repeated hepatectomy for frequent recurrence of hepatic metastasis from gastrointestinal stromal tumor of the stomach. Hepatogastroenterology. 2004; 51:181–183. PMID: 15011859.23. Demetri GD, von Mehren M, Blanke CD, Van den Abbeele AD, Eisenberg B, Roberts PJ, et al. Efficacy and safety of imatinib mesylate in advanced gastrointestinal stromal tumors. N Engl J Med. 2002; 347:472–480. PMID: 12181401.
Article24. Zhu J, Yang Y, Zhou L, Jiang M, Hou M. A long-term follow-up of the imatinib mesylate treatment for the patients with recurrent gastrointestinal stromal tumor (GIST): the liver metastasis and the outcome. BMC Cancer. 2010; 10:199. PMID: 20465813.
Article25. DeMatteo RP, Maki RG, Singer S, Gonen M, Brennan MF, Antonescu CR. Results of tyrosine kinase inhibitor therapy followed by surgical resection for metastatic gastrointestinal stromal tumor. Ann Surg. 2007; 245:347–352. PMID: 17435539.
Article26. Haller F, Detken S, Schulten HJ, Happel N, Gunawan B, Kuhlgatz J, et al. Surgical management after neoadjuvant imatinib therapy in gastrointestinal stromal tumours (GISTs) with respect to imatinib resistance caused by secondary KIT mutations. Ann Surg Oncol. 2007; 14:526–532. PMID: 17139461.
Article27. Demetri GD, van Oosterom AT, Garrett CR, Blackstein ME, Shah MH, Verweij J, et al. Efficacy and safety of sunitinib in patients with advanced gastrointestinal stromal tumour after failure of imatinib: a randomised controlled trial. Lancet. 2006; 368:1329–1338. PMID: 17046465.
Article28. Zalinski S, Palavecino M, Abdalla EK. Hepatic resection for gastrointestinal stromal tumor liver metastases. Hematol Oncol Clin North Am. 2009; 23:115–127. PMID: 19248975.
Article29. Rutkowski P, Nyckowski P, Grzesiakowska U, Nowecki ZI, Nasierowska-Guttmejer A, Pienkowski A, et al. The clinical characteristics and the role of surgery and imatinib treatment in patients with liver metastases from c-Kit positive gastrointestinal stromal tumors (GIST). Neoplasma. 2003; 50:438–442. PMID: 14689066.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Therapy of Pancreatic Neuroendocrine Tumors: Fine Needle Intervention including Ethanol and Radiofrequency Ablation
- Endoscopic ultrasound-guided ablation of pancreatic cystic lesions
- Recent Advances in the Image-Guided Tumor Ablation of Liver Malignancies: Radiofrequency Ablation with Multiple Electrodes, Real-Time Multimodality Fusion Imaging, and New Energy Sources
- Comparative analysis of Laparoscopic versus open surgical radiofrequency ablation for malignant liver tumors
- Radiofrequency Thermal Ablation of Hepatocellular Carcinomas
