Comparison of Chest Pain Protocols for Electrocardiography-Gated Dual-Source Cardiothoracic CT in Children and Adults: The Effect of Tube Current Saturation on Radiation Dose Reduction
- Affiliations
-
- 1Department of Radiology and Research Institute of Radiology, University of Ulsan College of Medicine, Asan Medical Center, Seoul 05505, Korea. ghw68@hanmail.net
- KMID: 2425105
- DOI: http://doi.org/10.3348/kjr.2018.19.1.23
Abstract
OBJECTIVE
To compare radiation doses between conventional and chest pain protocols using dual-source retrospectively electrocardiography (ECG)-gated cardiothoracic computed tomography (CT) in children and adults and assess the effect of tube current saturation on radiation dose reduction.
MATERIALS AND METHODS
This study included 104 patients (16.6 ± 7.7 years, range 5-48 years) that were divided into two groups: those with and those without tube current saturation. The estimated radiation doses of retrospectively ECG-gated spiral cardiothoracic CT were compared between conventional, uniphasic, and biphasic chest pain protocols acquired with the same imaging parameters in the same patients by using paired t tests. Dose reduction percentages, patient ages, volume CT dose index values, and tube current time products per rotation were compared between the two groups by using unpaired t tests. A p value < 0.05 was considered significant.
RESULTS
The volume CT dose index values of the biphasic chest pain protocol (10.8 ± 3.9 mGy) were significantly lower than those of the conventional protocol (12.2 ± 4.7 mGy, p < 0.001) and those of the uniphasic chest pain protocol (12.9 ± 4.9 mGy, p < 0.001). The dose-saving effect of biphasic chest pain protocol was significantly less with a saturated tube current (4.5 ± 10.2%) than with unsaturated tube current method (14.8 ± 11.5%, p < 0.001). In 76 patients using 100 kVp, patient age showed no significant differences between the groups with and without tube current saturation in all protocols (p > 0.05); the groups with tube current saturation showed significantly higher volume CT dose index values (p < 0.01) and tube current time product per rotation (p < 0.001) than the groups without tube current saturation in all protocols.
CONCLUSION
The radiation dose of dual-source retrospectively ECG-gated spiral cardiothoracic CT can be reduced by approximately 15% by using the biphasic chest pain protocol instead of the conventional protocol in children and adults if radiation dose parameters are further optimized to avoid tube current saturation.
Keyword
MeSH Terms
Figure
-
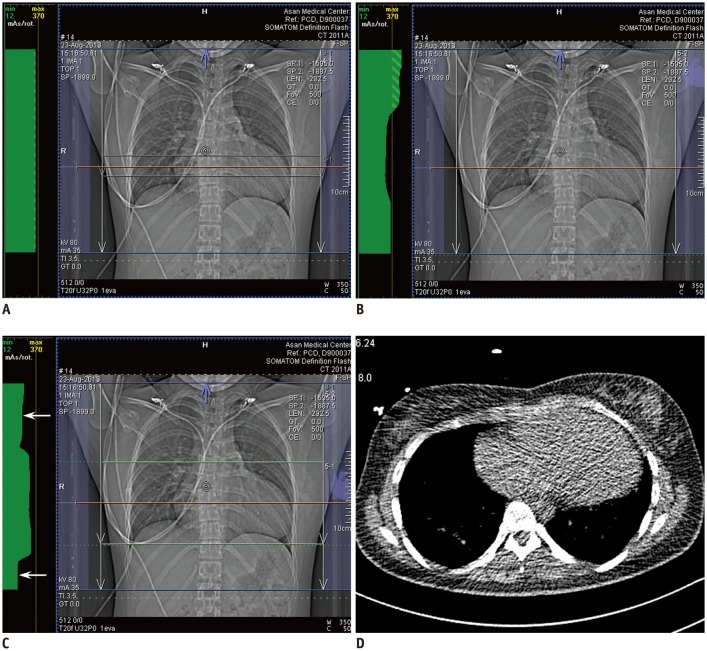
Fig. 1 Retrospectively ECG-gated spiral cardiothoracic CT using dual-source technique in 23-year-old woman with repaired tetralogy of Fallot.A. Anteroposterior scout image of conventional CT protocol shows tube current modulation curve in green throughout whole longitudinal scan range indicating no tube current saturation. In other words, tube current time product per rotation remains below maximum value of 370 over entire scanning range. Of note, tube current modulation curve is flat on top indicating no change in tube current time product per rotation over whole scan range in this protocol. B. Anteroposterior scout image of uniphasic chest pain CT protocol demonstrates tube current modulation curve in green over whole longitudinal scan range. In contrast to conventional CT protocol (A), tube current time product per rotation is modulated in this protocol according to patient-specific attenuation information acquired from scout image. C. Anteroposterior scout image of biphasic chest pain CT protocol also displays tube current modulation curve in green over whole longitudinal scan range. In this protocol, cardiac region is defined by user as green dotted lines and radiation dose is subsequently reduced to half (arrows) in upper and lower parts of scan range outside cardiac region because one of two X-ray tubes in dual-source CT system is switched off in these regions. D. From axial CT image acquired at slice position (orange line in A–C) approximately 2.5 cm above liver dome for bolus tracking, cross sectional area and mean body density was measured as 597 mm2 and −147 Hounsfield unit, respectively, and optimal volume CT dose index for non-ECG-synchronized cardiothoracic CT was calculated as 3.8 mGy (for one slice) that was increased to 4.8 mGy (for whole scan range) after application of automatic tube current modulation. Axial CT image looks noisy because low radiation dose setting (80 kVp and 25 mA) was used to minimize patient radiation exposure. CT = computed tomography, ECG = electrocardiography
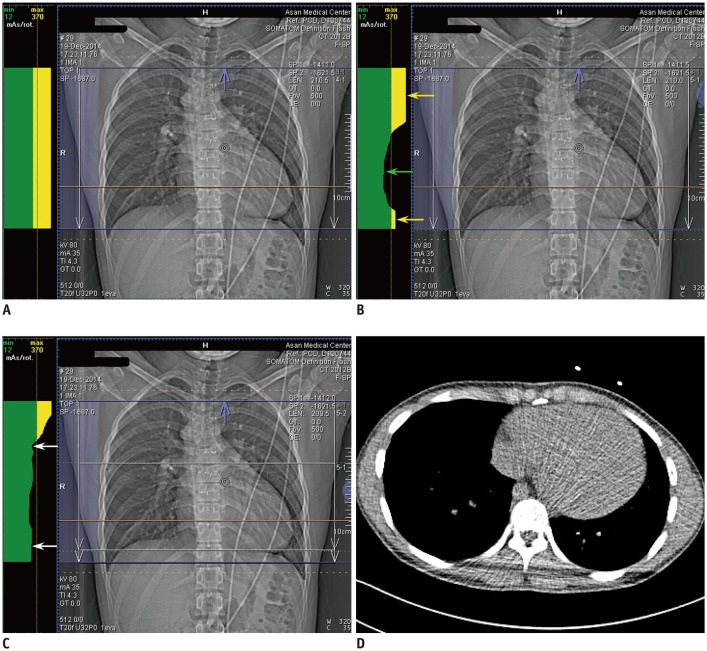
Fig. 2 Retrospectively ECG-gated spiral cardiothoracic CT using dual-source technique in 19-year-old man with repaired double-outlet right ventricle and subaortic ventricular septal defect.A. Anteroposterior scout image of conventional CT protocol shows upper part of tube current modulation curve in yellow throughout whole longitudinal scan range indicating tube current saturation. It means that tube current time product per rotation exceeds maximum value of 370 over entire scanning range. Of note, tube current modulation curve is flat on top indicating no change in tube current time product per rotation over whole scan range in this protocol. B. Anteroposterior scout image of uniphasic chest pain CT protocol demonstrates upper part of tube current modulation curve in yellow in upper thorax (yellow arrow) and lower thorax (yellow arrow) exceeding maximum tube current time product per rotation of 370. In contrast, tube current time product per rotation is modulated below maximum value of 370 in cardiac region (green arrow). C. Anteroposterior scout image of biphasic chest pain CT protocol shows that tube current time product per rotation is reduced (arrows) in upper and lower parts of scan range outside cardiac region defined by user as green dotted lines. Nonetheless, yellow tube current saturation is still shown in upper thorax. D. From axial CT image acquired at slice position (orange line in A–C) approximately 2.0 cm above liver dome for bolus tracking, cross sectional area and mean body density was measured as 522 mm2 and −240 Hounsfield unit, respectively, and optimal volume CT dose index for non-ECG-synchronized cardiothoracic CT was calculated as 2.8 mGy (for one slice) that was increased to 5.1 mGy (for whole scan range) after application of automatic tube current modulation. Axial CT image looks noisy because low radiation dose setting (80 kVp and 25 mA) was used to minimize patient radiation exposure.
Cited by 4 articles
-
Semiautomatic Three-Dimensional Threshold-Based Cardiac Computed Tomography Ventricular Volumetry in Repaired Tetralogy of Fallot: Comparison with Cardiac Magnetic Resonance Imaging
Hyun Woo Goo
Korean J Radiol. 2019;20(1):102-113. doi: 10.3348/kjr.2018.0237.Computed Tomography Pulmonary Vascular Volume Ratio Can Be Used to Evaluate the Effectiveness of Pulmonary Angioplasty in Peripheral Pulmonary Artery Stenosis
Hyun Woo Goo
Korean J Radiol. 2019;20(10):1422-1430. doi: 10.3348/kjr.2019.0286.User-Friendly Vendor-Specific Guideline for Pediatric Cardiothoracic Computed Tomography Provided by the Asian Society of Cardiovascular Imaging Congenital Heart Disease Study Group: Part 1. Imaging Techniques
Sun Hwa Hong, Hyun Woo Goo, Eriko Maeda, Ki Seok Choo, I-Chen Tsai,
Korean J Radiol. 2019;20(2):190-204. doi: 10.3348/kjr.2018.0571.Changes in Right Ventricular Volume, Volume Load, and Function Measured with Cardiac Computed Tomography over the Entire Time Course of Tetralogy of Fallot
Hyun Woo Goo
Korean J Radiol. 2019;20(6):956-966. doi: 10.3348/kjr.2018.0891.
Reference
-
1. Goo HW. State-of-the-art CT imaging techniques for congenital heart disease. Korean J Radiol. 2010; 11:4–18. PMID: 20046490.
Article2. Kakouros N, Giles J, Crundwell NB, McWilliams ET. The utility of cardiac CT beyond the assessment of suspected coronary artery disease. Clin Radiol. 2012; 67:695–708. PMID: 22316592.
Article3. Oda S, Utsunomiya D, Funama Y, Awai K, Katahira K, Nakaura T, et al. A low tube voltage technique reduces the radiation dose at retrospective ECG-gated cardiac computed tomography for anatomical and functional analyses. Acad Radiol. 2011; 18:991–999. PMID: 21536464.
Article4. Sommer WH, Albrecht E, Bamberg F, Schenzle JC, Johnson TR, Neumaier K, et al. Feasibility and radiation dose of high-pitch acquisition protocols in patients undergoing dual-source cardiac CT. AJR Am J Roentgenol. 2010; 195:1306–1312. PMID: 21098188.
Article5. Wang R, Schoepf UJ, Wu R, Gibbs KP, Yu W, Li M, et al. CT coronary angiography: image quality with sinogram-affirmed iterative reconstruction compared with filtered back-projection. Clin Radiol. 2013; 68:272–278. PMID: 22981731.
Article6. Koch K, Oellig F, Oberholzer K, Bender P, Kunz P, Mildenberger P, et al. Assessment of right ventricular function by 16-detector-row CT: comparison with magnetic resonance imaging. Eur Radiol. 2005; 15:312–318. PMID: 15565315.
Article7. Goo HW. Current trends in cardiac CT in children. Acta Radiol. 2013; 54:1055–1062. PMID: 23104372.
Article8. Goo HW, Park SH. Semiautomatic three-dimensional CT ventricular volumetry in patients with congenital heart disease: agreement between two methods with different user interaction. Int J Cardiovasc Imaging. 2015; 31(Suppl 2):223–232. PMID: 26319216.
Article9. Kim HJ, Goo HW, Park SH, Yun TJ. Left ventricle volume measured by cardiac CT in an infant with a small left ventricle: a new and accurate method in determining uni- or biventricular repair. Pediatr Radiol. 2013; 43:243–246. PMID: 22875206.
Article10. Hui PKT, Goo HW, Du J, Ip JJK, Kanzaki S, Kim YJ, et al. Asian consortium on radiation dose of pediatric cardiac CT (ASCI-REDCARD). Pediatr Radiol. 2017; 47:899–910. PMID: 28435986.
Article11. Johnson TR, Nikolaou K, Becker A, Leber AW, Rist C, Wintersperger BJ, et al. Dual-source CT for chest pain assessment. Eur Radiol. 2008; 18:773–780. PMID: 18034246.
Article12. Krissak R, Henzler T, Prechel A, Reichert M, Gruettner J, Sueselbeck T, et al. Triple-rule-out dual-source CT angiography of patients with acute chest pain: dose reduction potential of 100 kV scanning. Eur J Radiol. 2012; 81:3691–3696. PMID: 21163600.13. Goo HW. Individualized volume CT dose index determined by cross-sectional area and mean density of the body to achieve uniform image noise of contrast-enhanced pediatric chest CT obtained at variable kV levels and with combined tube current modulation. Pediatr Radiol. 2011; 41:839–847. PMID: 21656275.
Article14. Israel GM, Herlihy S, Rubinowitz AN, Cornfeld D, Brink J. Does a combination of dose modulation with fast gantry rotation time limit CT image quality? AJR Am J Roentgenol. 2008; 191:140–144. PMID: 18562737.
Article15. Goo HW, Suh DS. Tube current reduction in pediatric non-ECG-gated heart CT by combined tube current modulation. Pediatr Radiol. 2006; 36:344–351. PMID: 16501970.
Article16. Goo HW, Suh DS. The influences of tube voltage and scan direction on combined tube current modulation: a phantom study. Pediatr Radiol. 2006; 36:833–840. PMID: 16642311.
Article17. Sommer WH, Schenzle JC, Becker CR, Nikolaou K, Graser A, Michalski G, et al. Saving dose in triple-rule-out computed tomography examination using a high-pitch dual spiral technique. Invest Radiol. 2010; 45:64–71. PMID: 20027121.
Article18. Bamberg F, Marcus R, Sommer W, Schwarz F, Nikolaou K, Becker CR, et al. Diagnostic image quality of a comprehensive high-pitch dual-spiral cardiothoracic CT protocol in patients with undifferentiated acute chest pain. Eur J Radiol. 2012; 81:3697–3702. PMID: 21196093.
Article19. Pursnani A, Lee A, Mayrhofer T, Panagia M, Sharma U, Abbara S, et al. Feasibility of a radiation dose conserving CT protocol for myocardial function assessment. Br J Radiol. 2014; 87:20130755. PMID: 24884727.
Article20. Ketelsen D, Luetkhoff MH, Thomas C, Werner M, Buchgeister M, Tsiflikas I, et al. Estimation of the radiation exposure of a chest pain protocol with ECG-gating in dual-source computed tomography. Eur Radiol. 2009; 19:37–41. PMID: 18648818.
Article21. Niemann T, Henry S, Faivre JB, Yasunaga K, Bendaoud S, Simeone A, et al. Clinical evaluation of automatic tube voltage selection in chest CT angiography. Eur Radiol. 2013; 23:2643–2651. PMID: 23828227.
Article22. Shin HJ, Chung YE, Lee YH, Choi JY, Park MS, Kim MJ, et al. Radiation dose reduction via sinogram affirmed iterative reconstruction and automatic tube voltage modulation (CARE kV) in abdominal CT. Korean J Radiol. 2013; 14:886–893. PMID: 24265563.
Article23. Mayer C, Meyer M, Fink C, Schmidt B, Sedlmair M, Schoenberg SO, et al. Potential for radiation dose savings in abdominal and chest CT using automatic tube voltage selection in combination with automatic tube current modulation. AJR Am J Roentgenol. 2014; 203:292–299. PMID: 25055262.
Article24. Lee E, Goo HW, Lee JY. Age- and gender-specific estimates of cumulative CT dose over 5 years using real radiation dose tracking data in children. Pediatr Radiol. 2015; 45:1282–1292. PMID: 25801905.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Image Quality and Radiation Dose of High-Pitch Dual-Source Spiral Cardiothoracic Computed Tomography in Young Children with Congenital Heart Disease: Comparison of Non-Electrocardiography Synchronization and Prospective Electrocardiography Triggering
- Is It Better to Enter a Volume CT Dose Index Value before or after Scan Range Adjustment for Radiation Dose Optimization of Pediatric Cardiothoracic CT with Tube Current Modulation?
- Comparison of Radiation Dose and Image Quality between the 2nd Generation and 3rd Generation Dual-Source Single-Energy and Dual-Source Dual-Energy CT of the Abdomen
- Prospectively Electrocardiogram-Gated High-Pitch Spiral Acquisition Mode Dual-Source CT Coronary Angiography in Patients with High Heart Rates: Comparison with Retrospective Electrocardiogram-Gated Spiral Acquisition Mode
- Effects of Iterative Reconstruction Algorithm, Automatic Exposure Control on Image Quality, and Radiation Dose: Phantom Experiments with Coronary CT Angiography Protocols
