Prospectively Electrocardiogram-Gated High-Pitch Spiral Acquisition Mode Dual-Source CT Coronary Angiography in Patients with High Heart Rates: Comparison with Retrospective Electrocardiogram-Gated Spiral Acquisition Mode
- Affiliations
-
- 1Department of Radiology, Baotou Central Hospital, Baotou 014040, China. henrysk@163.com
- 2Department of Cardiology, Baotou Central Hospital, Baotou 014040, China.
- 3CT BM Clinic Marketing, Siemens Healthcare, Beijing 100102, China.
- KMID: 1397498
- DOI: http://doi.org/10.3348/kjr.2012.13.6.684
Abstract
OBJECTIVE
To assess the image quality and effective radiation dose of prospectively electrocardiogram (ECG)-gated high-pitch spiral acquisition mode (flash mode) of dual-source CT (DSCT) coronary angiography (CTCA) in patients with high heart rates (HRs) as compared with retrospectively ECG-gated spiral acquisition mode.
MATERIALS AND METHODS
Two hundred and sixty-eight consecutive patients (132 female, mean age: 55 +/- 11 years) with mean HR > 65 beats per minute (bpm) were prospectively included in this study. The patients were divided into two groups. Collection was performed in group A CTCA using flash mode setting at 20-30% of the R-R interval, and retrospectively ECG-gated spiral acquisition mode in group B. The image noise, contrast-to-noise ratio (CNR), image quality scores, effective radiation dose and influencing factors on image quality between the two groups were assessed.
RESULTS
There were no significant differences in image quality scores and proportions of non-diagnostic coronary artery segments between two groups (image quality scores: 1.064 +/- 0.306 [group A] vs. 1.084 +/- 0.327 [group B], p = 0.063; proportion of non-diagnostic coronary artery segments: segment-based analysis 1.52% (group A) vs. 1.74% (group B), p = 0.345; patient-based analysis 7.5% (group A) vs. 6.7% (group B), p = 0.812). The estimated radiation dose was 1.0 +/- 0.16 mSv in group A and 7.1 +/- 1.05 mSv in group B (p = 0.001).
CONCLUSION
In conclusion, in patients with HRs > 65 bpm without cardiac arrhythmia, the prospectively high-pitch spiral-acquisition mode with image-acquired timing set at 20-30% of the R-R interval provides a similar image quality and low rate of non-diagnostic coronary segments to the retrospectively ECG-gated low-pitch spiral acquisition mode, with significant reduction of radiation exposure.
MeSH Terms
Figure
-

Fig. 1 HP dual-source computed tomography coronary angiography in 55-year-old woman (heart rate: 99 bpm) from Group A. Electrocardiogram signal (A) demonstrates depiction of entire heart within single heart beat. Curved reformations of right coronary artery (B), left anterior descending artery (C) and left circumflex artery (D) did not show motion artifacts (score 1). Image quality was classified as excellent (i.e. score 1) in all coronary segments. RCA = right coronary artery, LCX = left circumflex artery

Fig. 2 HP dual-source computed tomography coronary angiography in 40-year-old man (heart rate: 79 bpm) from group A. Electrocardiogram signal (A) demonstrates that high-pitch spiral mode in acquisition at 20% of R-R interval falls into scan range of R wave because HR variability was too high (26 bpm). Motion artifacts occurred at right coronary artery (B, C) and left circumflex artery (D) (score 3). LCX = left circumflex artery
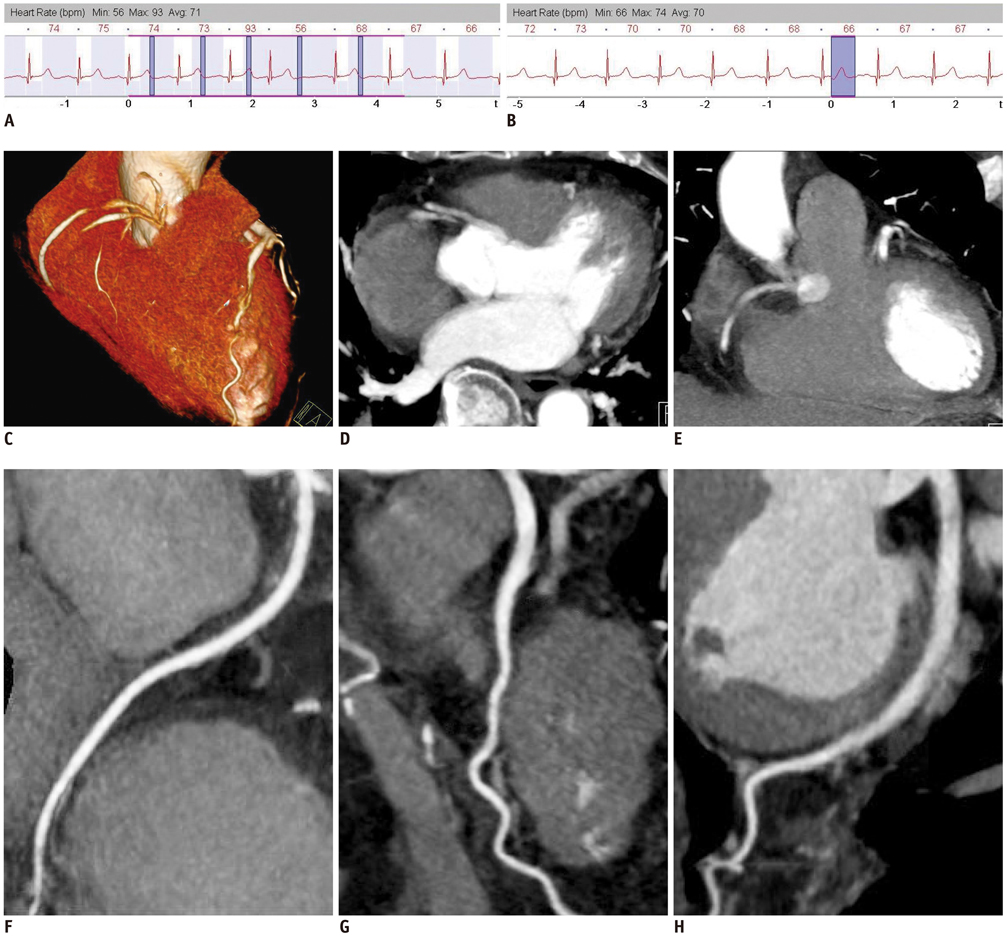
Fig. 3 47-year-old woman (heart rate: 70 bpm) underwent CTCA. Image is not evaluative and vessels are not differentiable due to effect of respiration using spiral mode (B, C, D). High-pitch spiral mode in acquisition at 20% of R-R interval CTCA was used, and patient had diagnostic evaluation of entire coronary artery tree (F, G, H). Electrocardiogram signal (A, E) demonstrated acquisition window of spiral mode and high-pitch spiral mode. CTCA = computed tomography coronary angiography, LAD = left anterior descending artety, LCX = left circumflex artery
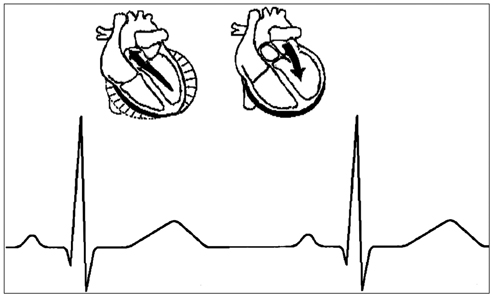
Fig. 4 Most important features of cardiac cycle and optimal scan time of flash mode computed tomography coronary angiography within single heart beat.
Reference
-
1. Husmann L, Herzog BA, Burger IA, Buechel RR, Pazhenkottil AP, von Schulthess P, et al. Usefulness of additional coronary calcium scoring in low-dose CT coronary angiography with prospective ECG-triggering impact on total effective radiation dose and diagnostic accuracy. Acad Radiol. 2010. 17:201–206.2. Ropers D, Pohle FK, Kuettner A, Pflederer T, Anders K, Daniel WG, et al. Diagnostic accuracy of noninvasive coronary angiography in patients after bypass surgery using 64-slice spiral computed tomography with 330-ms gantry rotation. Circulation. 2006. 114:2334–2341. quiz 2334.3. Carrascosa P, Capuñay C, Deviggiano A, Goldsmit A, Tajer C, Bettinotti M, et al. Accuracy of low-dose prospectively gated axial coronary CT angiography for the assessment of coronary artery stenosis in patients with stable heart rate. J Cardiovasc Comput Tomogr. 2010. 4:197–205.4. Xu Y, Tang L, Zhu X, Xu H, Tang J, Yang Z, et al. Comparison of dual-source CT coronary angiography and conventional coronary angiography for detecting coronary artery disease. Int J Cardiovasc Imaging. 2010. 26:Suppl 1. 75–81.5. Zhang LJ, Wu SY, Wang J, Lu Y, Zhang ZL, Jiang SS, et al. Diagnostic accuracy of dual-source CT coronary angiography: the effect of average heart rate, heart rate variability, and calcium score in a clinical perspective. Acta Radiol. 2010. 51:727–740.6. Moon JH, Park EA, Lee W, Yin YH, Chung JW, Park JH, et al. The diagnostic accuracy, image quality and radiation dose of 64-slice dual-source CT in daily practice: a single institution's experience. Korean J Radiol. 2011. 12:308–318.7. Hausleiter J, Meyer T, Hermann F, Hadamitzky M, Krebs M, Gerber TC, et al. Estimated radiation dose associated with cardiac CT angiography. JAMA. 2009. 301:500–507.8. Scheffel H, Alkadhi H, Leschka S, Plass A, Desbiolles L, Guber I, et al. Low-dose CT coronary angiography in the step-and-shoot mode: diagnostic performance. Heart. 2008. 94:1132–1137.9. Achenbach S, Goroll T, Seltmann M, Pflederer T, Anders K, Ropers D, et al. Detection of coronary artery stenoses by low-dose, prospectively ECG-triggered, high-pitch spiral coronary CT angiography. JACC Cardiovasc Imaging. 2011. 4:328–337.10. Alkadhi H, Stolzmann P, Desbiolles L, Baumueller S, Goetti R, Plass A, et al. Low-dose, 128-slice, dual-source CT coronary angiography: accuracy and radiation dose of the high-pitch and the step-and-shoot mode. Heart. 2010. 96:933–938.11. Leschka S, Stolzmann P, Desbiolles L, Baumueller S, Goetti R, Schertler T, et al. Diagnostic accuracy of high-pitch dual-source CT for the assessment of coronary stenoses: first experience. Eur Radiol. 2009. 19:2896–2903.12. Wang YN, Li L, Kong LY, Wang ZW, Zhou K, Cao J, et al. [Coronary computed tomographic angiography using low-dose prospectively electrocardiographic triggered high-pitch spiral acquisition by dual-source computed tomography: image quality and radiation dose]. Zhongguo Yi Xue Ke Xue Yuan Xue Bao. 2010. 32:597–600.13. Seifarth H, Wienbeck S, Püsken M, Juergens KU, Maintz D, Vahlhaus C, et al. Optimal systolic and diastolic reconstruction windows for coronary CT angiography using dual-source CT. AJR Am J Roentgenol. 2007. 189:1317–1323.14. Weustink AC, Mollet NR, Pugliese F, Meijboom WB, Nieman K, Heijenbrok-Kal MH, et al. Optimal electrocardiographic pulsing windows and heart rate: effect on image quality and radiation exposure at dual-source coronary CT angiography. Radiology. 2008. 248:792–798.15. Araoz PA, Kirsch J, Primak AN, Braun NN, Saba O, Williamson EE, et al. Optimal image reconstruction phase at low and high heart rates in dual-source CT coronary angiography. Int J Cardiovasc Imaging. 2009. 25:837–845.16. Goetti R, Feuchtner G, Stolzmann P, Desbiolles L, Fischer MA, Karlo C, et al. High-pitch dual-source CT coronary angiography: systolic data acquisition at high heart rates. Eur Radiol. 2010. 20:2565–2571.17. Halliburton SS, Sola S, Kuzmiak SA, Obuchowski NA, Desai M, Flamm SD, et al. Effect of dual-source cardiac computed tomography on patient radiation dose in a clinical setting: comparison to single-source imaging. J Cardiovasc Comput Tomogr. 2008. 2:392–400.18. Lell M, Marwan M, Schepis T, Pflederer T, Anders K, Flohr T, et al. Prospectively ECG-triggered high-pitch spiral acquisition for coronary CT angiography using dual source CT: technique and initial experience. Eur Radiol. 2009. 19:2576–2583.19. Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, Griffith LS, et al. A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc Committee for Grading of Coronary Artery Disease, Council on Cardiovascular Surgery, American Heart Association. Circulation. 1975. 51:5–40.20. Qi W, Li J, Du X. Method for automatic tube current selection for obtaining a consistent image quality and dose optimization in a cardiac multidetector CT. Korean J Radiol. 2009. 10:568–574.21. Menzel HG, Schibilla H, Teunen D, editors. Publication no. EUR 16262 EN. European guidelines on quality criteria for computed tomography. 2000. Luxembourg: European Commission.22. Wolf F, Leschka S, Loewe C, Homolka P, Plank C, Schernthaner R, et al. Coronary artery stent imaging with 128-slice dual-source CT using high-pitch spiral acquisition in a cardiac phantom: comparison with the sequential and low-pitch spiral mode. Eur Radiol. 2010. 20:2084–2091.23. Goo HW. State-of-the-art CT imaging techniques for congenital heart disease. Korean J Radiol. 2010. 11:4–18.24. Duarte R, Fernandez G, Castellon D, Costa JC. Prospective Coronary CT Angiography 128-MDCT Versus Retrospective 64-MDCT: Improved Image Quality and Reduced Radiation Dose. Heart Lung Circ. 2011. 20:119–125.25. Hirai N, Horiguchi J, Fujioka C, Kiguchi M, Yamamoto H, Matsuura N, et al. Prospective versus retrospective ECG-gated 64-detector coronary CT angiography: assessment of image quality, stenosis, and radiation dose. Radiology. 2008. 248:424–430.26. Earls JP, Berman EL, Urban BA, Curry CA, Lane JL, Jennings RS, et al. Prospectively gated transverse coronary CT angiography versus retrospectively gated helical technique: improved image quality and reduced radiation dose. Radiology. 2008. 246:742–753.27. Raff GL, Gallagher MJ, O'Neill WW, Goldstein JA. Diagnostic accuracy of noninvasive coronary angiography using 64-slice spiral computed tomography. J Am Coll Cardiol. 2005. 46:552–557.28. Rixe J, Rolf A, Conradi G, Elsaesser A, Moellmann H, Nef HM, et al. Image quality on dual-source computed-tomographic coronary angiography. Eur Radiol. 2008. 18:1857–1862.29. Stolzmann P, Leschka S, Scheffel H, Krauss T, Desbiolles L, Plass A, et al. Dual-source CT in step-and-shoot mode: noninvasive coronary angiography with low radiation dose. Radiology. 2008. 249:71–80.30. Scheffel H, Alkadhi H, Plass A, Vachenauer R, Desbiolles L, Gaemperli O, et al. Accuracy of dual-source CT coronary angiography: First experience in a high pre-test probability population without heart rate control. Eur Radiol. 2006. 16:2739–2747.31. Achenbach S, Ropers D, Holle J, Muschiol G, Daniel WG, Moshage W. In-plane coronary arterial motion velocity: measurement with electron-beam CT. Radiology. 2000. 216:457–463.32. Adler G, Meille L, Rohnean A, Sigal-Cinqualbre A, Capderou A, Paul JF. Robustness of end-systolic reconstructions in coronary dual-source CT angiography for high heart rate patients. Eur Radiol. 2010. 20:1118–1123.33. Guyer S. Cardiovascular physiology as a basis for clinical and financial outcomes. J Cardiovasc Manag. 1998. 9:20–24.34. Tsakiris S, Zarros A. Medical physiology and experimentation: reconsidering the undergraduate examination structure. Adv Physiol Educ. 2006. 30:94–95.35. Alonso Guerrero A. [Cardiac physiology]. Rev Enferm. 1983. 6:49–54.36. Saffitz JE. Dependence of electrical coupling on mechanical coupling in cardiac myocytes: insights gained from cardiomyopathies caused by defects in cell-cell connections. Ann N Y Acad Sci. 2005. 1047:336–344.37. Leschka S, Wildermuth S, Boehm T, Desbiolles L, Husmann L, Plass A, et al. Noninvasive coronary angiography with 64-section CT: effect of average heart rate and heart rate variability on image quality. Radiology. 2006. 241:378–385.38. Weustink AC, Neefjes LA, Kyrzopoulos S, van Straten M, Neoh Eu R, Meijboom WB, et al. Impact of heart rate frequency and variability on radiation exposure, image quality, and diagnostic performance in dual-source spiral CT coronary angiography. Radiology. 2009. 253:672–680.39. Herzog BA, Husmann L, Burkhard N, Gaemperli O, Valenta I, Tatsugami F, et al. Accuracy of low-dose computed tomography coronary angiography using prospective electrocardiogram-triggering: first clinical experience. Eur Heart J. 2008. 29:3037–3042.40. Maruyama T, Takada M, Hasuike T, Yoshikawa A, Namimatsu E, Yoshizumi T. Radiation dose reduction and coronary assessability of prospective electrocardiogram-gated computed tomography coronary angiography: comparison with retrospective electrocardiogram-gated helical scan. J Am Coll Cardiol. 2008. 52:1450–1455.41. Husmann L, Valenta I, Gaemperli O, Adda O, Treyer V, Wyss CA, et al. Feasibility of low-dose coronary CT angiography: first experience with prospective ECG-gating. Eur Heart J. 2008. 29:191–197.42. Alkadhi H, Stolzmann P, Scheffel H, Desbiolles L, Baumüller S, Plass A, et al. Radiation dose of cardiac dual-source CT: the effect of tailoring the protocol to patient-specific parameters. Eur J Radiol. 2008. 68:385–391.43. Achenbach S, Marwan M, Ropers D, Schepis T, Pflederer T, Anders K, et al. Coronary computed tomography angiography with a consistent dose below 1 mSv using prospectively electrocardiogram-triggered high-pitch spiral acquisition. Eur Heart J. 2010. 31:340–346.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Image Quality and Radiation Dose of High-Pitch Dual-Source Spiral Cardiothoracic Computed Tomography in Young Children with Congenital Heart Disease: Comparison of Non-Electrocardiography Synchronization and Prospective Electrocardiography Triggering
- Technical Aspect of Coronary CT Angiography: Imaging Tips and Safety Issues
- Initial Clinical Experience With Coronary CT Angiography Performed on Dual Source Photon Counting CT Using Different Cardiac Scan Modes-Analysis of Image Quality and Radiation Dose
- Giant coronary aneurysm caused by Kawasaki disease: consistency between catheter angiography and electrocardiogram gated dual-source computed tomography angiography
- Comparison of Chest Pain Protocols for Electrocardiography-Gated Dual-Source Cardiothoracic CT in Children and Adults: The Effect of Tube Current Saturation on Radiation Dose Reduction
