Imaging Features of Inflammatory Breast Disorders: A Pictorial Essay
- Affiliations
-
- 1Department of Diagnostic Radiology, Tan Tock Seng Hospital, Jalan Tan Tock Seng, Singapore 308433, Singapore. powey@hotmail.com
- 2Princess Margaret Hospital, Department of Medical Imaging, Toronto, ON M5G 2M9, Canada.
- KMID: 2425103
- DOI: http://doi.org/10.3348/kjr.2018.19.1.5
Abstract
- Inflammatory breast disorders include a wide array of underlying causes, ranging from common benign infection, non-infectious inflammation and inflammation resulting from underlying breast malignancy. Because it is at times difficult to distinguish mastitis and breast cancer based on clinical features, awareness of detailed imaging features may be helpful for better management of inflammatory breast disorders. Therefore, this pictorial essay intends to demonstrate radiologic findings of a variety of inflammatory breast disorders, using selected cases with mammography, ultrasound and magnetic resonance images.
Keyword
MeSH Terms
Figure
-
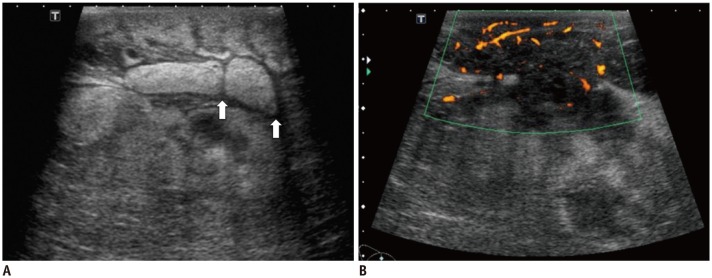
Fig. 1 Pueperal Mastitis in 29-year-old female.A. Ultrasound reveals features of subcutaneous edema with skin thickening with increase in echogenicity of subcutaneous tissue. Fluid is observed as intervening hypoechoic lines (white arrows) in subcutaneous tissue. B. Ultrasound with color Doppler also reveals ill-defined hypoechoic fluid collection with heterogeneous content within site of inflammation. Hyperemia of subcutaneous tissue surrounding collection is noted.
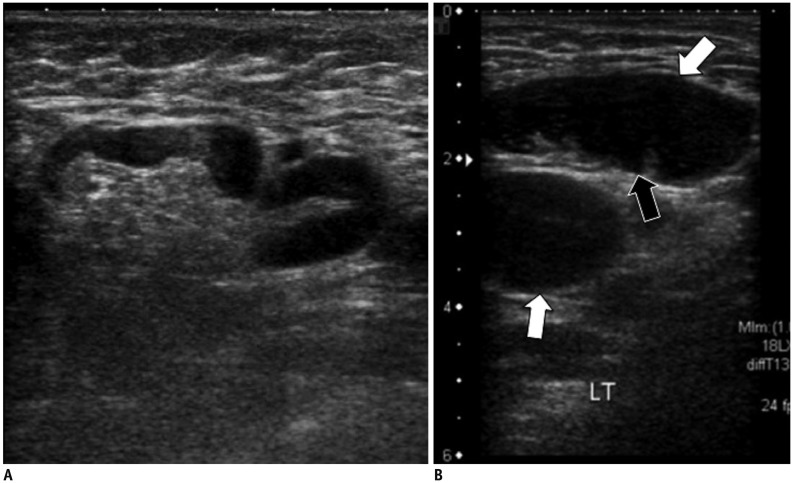
Fig. 2 Reactive versus malignant lymphadenopathy.A. Ultrasound of right axilla in 33-year-old female with large right breast abscess reveals enlarged lymph node with smooth thickening of cortex. Normal fatty hilum and reniform configuration is preserved. These are features of benign reactive lymph node. B. Ultrasound of right axilla in 52-year-old female, with painful right breast mass and palpable right axillary nodes. Lymph nodes reveal bulky cortex (white arrows) and loss of normal fatty hilum (black arrow), features that are more worrisome for malignant involvement. Ultrasound-guided biopsy of node was conducted and diagnosis of lymphoma was made.
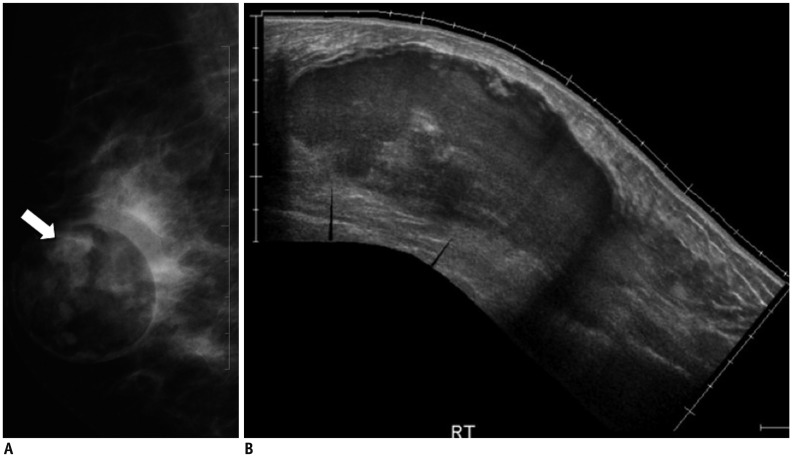
Fig. 3 Infected galactocele in 32-year-old lactating female presenting with right breast swelling and pain.A. Mammogram of right breast in mediolateral oblique projection shows well-defined predominantly lucent mass with some opaque material within (white arrow). This appearance is in keeping with presence of both lucent fat and dense proteinaceous content (milk and inflammatory cells). B. Ultrasound demonstrates large collection in right breast with heterogeneous cystic-solid content. This lesion was aspirated which yielded milk content and inflammatory cells. No malignant cell was observed. Subsequent follow-up ultrasound examinations reveal gradual resolution of this lesion.
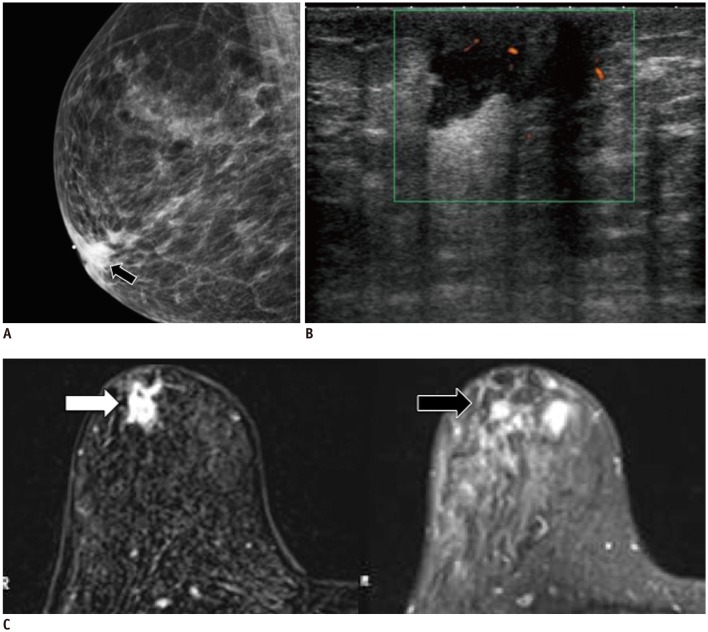
Fig. 4 Non-pueperal subareolar abscess in 49-year-old female with history of smoking.This patient presented with palpable retroareolar lump in right breast.A. Mammogram of right breast in mediolateral oblique projections reveals retro-areolar opacity (black arrow). B. Ultrasound reveals retro-areolar collection with increased peripheral vascularity in right breast. C. T2 weighted and post-contrast T1-weighted MR imaging shows cystic lesion in subareolar region of right breast on T2-weighted image (white arrow). This also demonstrates rim enhancement on post-contrast T1-weighted image (black arrow). Repeat ultrasound study conducted three months later reveals slightly smaller but persistent subareolar collection. This lesion was biopsied and inflammatory cells were seen. No malignant cells were obtained.
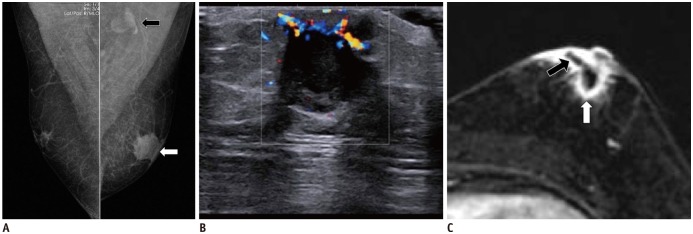
Fig. 5 Subaerolar abscess in 49-year-old male, presenting with left breast pain and swelling.A. Mammogram of both breasts in mediolateral oblique projections demonstrates left breast retro-areolar opacity (white arrow). Prominent left axillary node is also seen (black arrow). B. Ultrasound of left breast with color Doppler reveals hypoechoic collection in left subareolar region with echogenic internal debris and increased peripheral vascularity. Ultrasound guided tru-cut biopsy of this lesion was conducted which yielded inflammatory cells. No malignant cells were observed. C. Post contrast T1 weighted fat saturated MR imaging of both breasts in axial plane reveals subareolar rim-enhancing collection in left breast (white arrow). Fistulous tract extending to skin surface was also noted (black arrow).
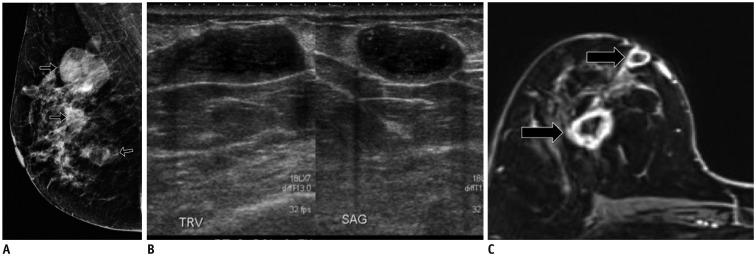
Fig. 6 Peripheral breast abscesses from infected cysts in 38-year-old non-lactating female, presenting with painful lumps in right breast.A. Mammogram of right breast reveals several partial circumscribed masses (black arrows), predominantly in upper half of right breast. B. Ultrasound of right breast reveals cysts with thickened walls and internal echogenic material. C. T1-weighted post contrast fat saturated MR imaging of breasts reveal presence of several cysts in upper half of right breast with thickened enhancing walls (black arrows). SAG = sagittal, TRV = transverse
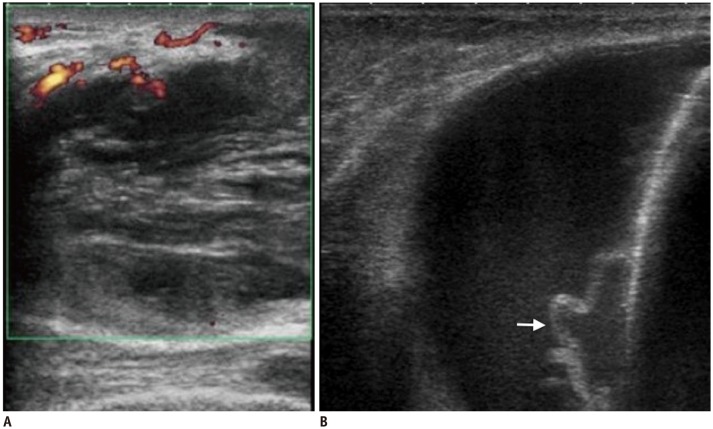
Fig. 7 Post-procedural breast infections.A. Post nipple-piercing breast abscess. This is immunocompromised 20-year-old female who presented with left breast swelling and pain post nipple piercing. Ultrasound image of left breast with color Doppler shows hypoechoic collection with heterogeneous content and increased peripheral vascularity. B. Abscess post mastectomy with insertion of tissue expander. This 62-year-old female experienced pain, redness and swelling after mastectomy with insertion of tissue expander. Ultrasound image of affected right breast reveals thick walled, lobulated collection situated posterior to tissue expander (white arrow). Aspiration of this lesion yielded inflammatory cells. No sign of malignant cells was observed.
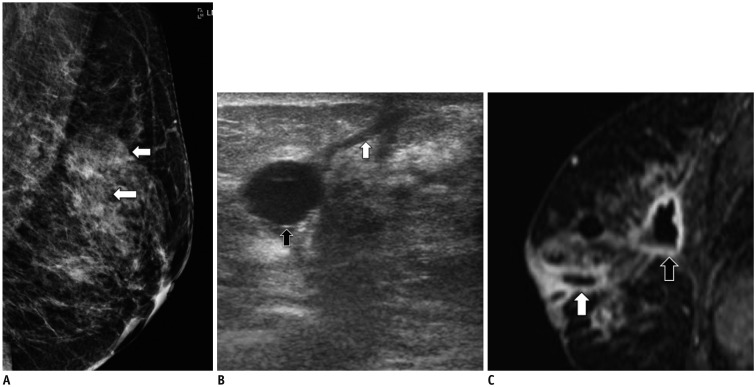
Fig. 8 Tuberculosis mastitis in 33-year-old female with chronic discharging sinuses in left breast.A. Mammogram of left breast demonstrates partially circumscribed masses in left breast (white arrows). B. Ultrasound of left breast reveals collections (black arrow) with fistulous tracts to skin surface (white arrow). C. T1-weighted fat saturated MR imaging of left breast in sagittal plane shows rim-enhancing collections (black arrow) with fistulous tracts to skin surface (white arrow). US-guided biopsy of these lesions revealed presence of acid-fast bacilli, in keeping with diagnosis of tuberculous mastitis. Chest radiograph was also conducted for this patient. However it did not reveal any sign of infection.
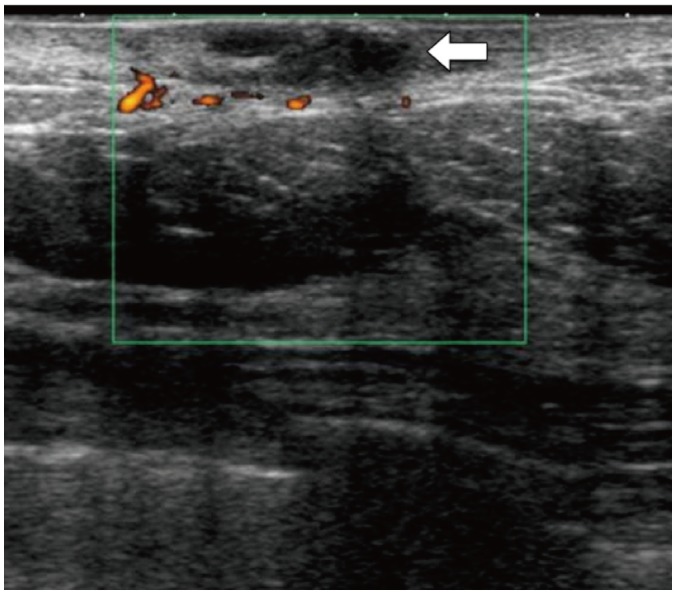
Fig. 9 Infected sebaceous cyst in 59-year-old female with painful left breast lump.Ultrasound of left breast with color Doppler reveals hypoechoic lesion within dermis with surrounding increased vascularity (white arrow). No deep extension of this lesion is observed. Surrounding skin is thickened.
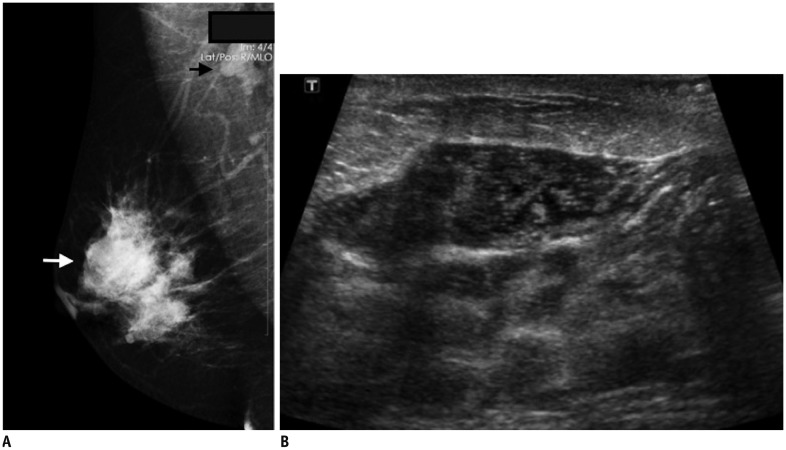
Fig. 10 Chronic granulomatous mastitis in 40-year-old female with long standing right breast pain and swelling.A. Mammogram of breasts in mediolateral oblique projection shows ill-defined mass in upper half of right breast (white arrow). There is also enlarged right axillary node (black arrow). B. Ultrasound examination reveals lobulated heterogeneously hypoechoic lesion in upper half of right breast. This lesion has imaging features that are suspicious for malignancy and ultrasound guided biopsy was conducted. Histological diagnosis of chronic granulomatous mastitis was made.
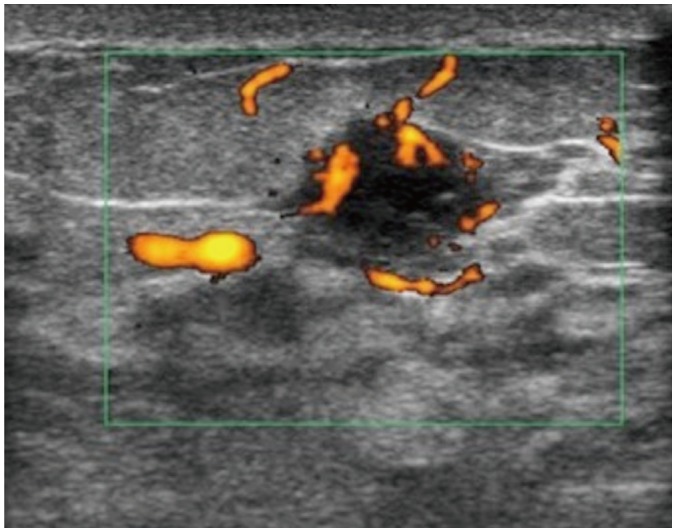
Fig. 11 Xanthogranulomatous mastitis in 41-year old female 34 weeks pregnant with pain in upper inner quadrant of left breast.Hypoechoic well-circumscribed lesion was seen in 2:00 position of left breast with surrounding and internal increased vascularity. This was thought to be likely related to lactational changes. However, due to presence of increased vascularity, this lesion was biopsied and histology revealed xanthogranulomatous mastitis.
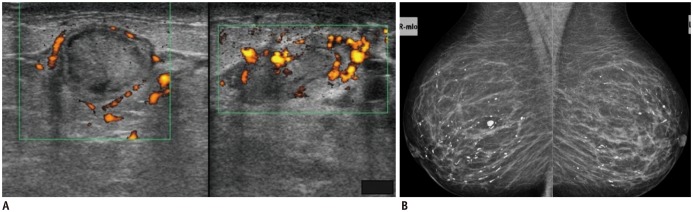
Fig. 12 Plasma cell mastitis.A. Plasma cell mastitis in non-lactating 34-year-old female with pain and swelling in lower half of left breast and nipple discharge. Ultrasound images of left breast in transverse (image on left) and longitudinal views (image on right) reveal markedly dilated intramammary duct in retroareolar region with echogenic content and surrounding increased vascularity. Ultrasound-guided biopsy of this duct was conducted to rule out malignancy, which only yielded inflammatory cells. B. Plasma cell mastitis in asymptomatic 71-year-old female at screening mammogram. Mammogram of both breasts in mediolateral oblique view shows characteristic large rod-like branching calcifications in both breasts.
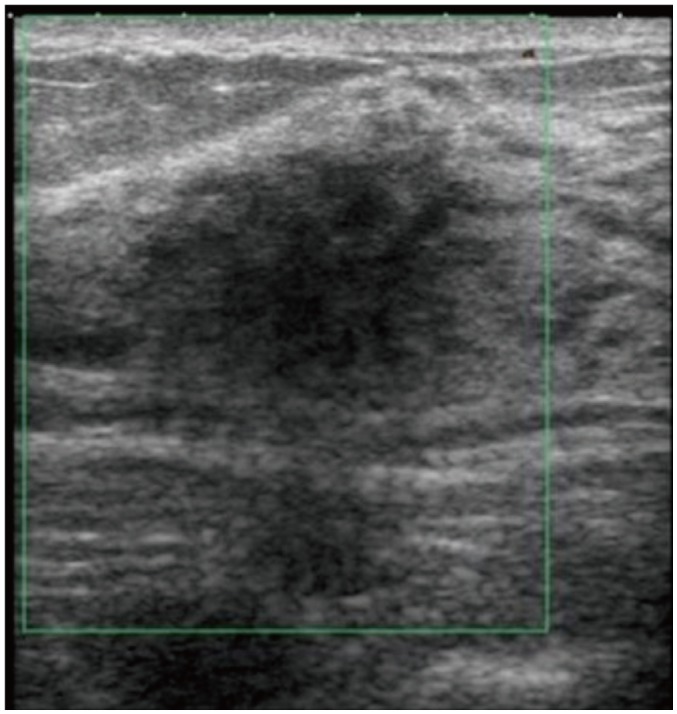
Fig. 13 Diabetic mastopathy in 29-year-old female with Type I diabetes, presenting with palpable lumps in upper outer quadrants of both breasts.Ultrasound of upper half of left breast reveals ill-defined heterogeneously hypoechoic area, with posterior acoustic shadowing. Similar findings were also observed over right breast.

Fig. 14 Inflammatory breast carcinoma in 43-year-old, presenting with right breast lump, pain and erythema with yellow nipple discharge and palpable right axillary lymph nodes.A. Mammogram of both breasts in mediolateral oblique view demonstrates ill-defined opacity on lower half of right breast (black arrows) with overlying skin thickening (white arrows). B. Ultrasound of right breast reveals heterogeneously hypoechoic, solid-cystic mass with increased peripheral vascularity. C. Enlarged right axillary node is observed with loss of normal fatty hilum and thickened cortex. US-guided biopsy was conducted on right breast mass and axillary node. Histology confirms presence of invasive carcinoma with ductal features.
Reference
-
1. Lepori D. Inflammatory breast disease: The radiologist's role. Diagn Interv Imaging. 2015; 96:1045–1064. PMID: 26372222.
Article2. Kasales CJ, Han B, Smith JS Jr, Chetlen AL, Kaneda HJ, Shereef S. Nonpuerperal mastitis and subareolar abscess of the breast. AJR Am J Roentgenol. 2014; 202:W133–W139. PMID: 24450694.
Article3. Kamal RM, Hamed ST, Salem DS. Classification of inflammatory breast disorders and step by step diagnosis. Breast J. 2009; 15:367–380. PMID: 19496780.
Article4. Tan H, Li R, Peng W, Liu H, Gu Y, Shen X. Radiological and clinical features of adult non-puerperal mastitis. Br J Radiol. 2013; 86:20120657. PMID: 23392197.
Article5. Kwak JY, Kim EK, Chung SY, You JK, Oh KK, Lee YH, et al. Unilateral breast edema: spectrum of etiologies and imaging appearances. Yonsei Med J. 2005; 46:1–7. PMID: 15744799.
Article6. Michie C, Lockie F, Lynn W. The challenge of mastitis. Arch Dis Child. 2003; 88:818–821. PMID: 12937109.
Article7. Kim YR, Kim HS, Kim HW. Are irregular hypoechoic breast masses on ultrasound always malignancies?: a pictorial essay. Korean J Radiol. 2015; 16:1266–1275. PMID: 26576116.
Article8. Sabate JM, Clotet M, Torrubia S, Gomez A, Guerrero R, de las Heras P, et al. Radiologic evaluation of breast disorders related to pregnancy and lactation. Radiographics. 2007; 27(Suppl 1):S101–S124. PMID: 18180221.
Article9. Gunawardena RP, Gunawardena D, Metcalf C, Taylor D, Wylie L. Inflammatory breast disease: a pictorial essay with radiological-pathological correlation. J Med Imaging Radiat Oncol. 2017; 61:70–76. PMID: 27324090.
Article10. Trop I, Dugas A, David J, El Khoury M, Boileau JF, Larouche N, et al. Breast abscesses: evidence-based algorithms for diagnosis, management, and follow-up. Radiographics. 2011; 31:1683–1699. PMID: 21997989.
Article11. Baharoon S. Tuberculosis of the breast. Ann Thorac Med. 2008; 3:110–114. PMID: 19561892.
Article12. Sabaté JM, Clotet M, Gómez A, De Las Heras P, Torrubia S, Salinas T. Radiologic evaluation of uncommon inflammatory and reactive breast disorders. Radiographics. 2005; 25:411–424. PMID: 15798059.
Article13. Gao Y, Slanetz PJ, Eisenberg RL. Echogenic breast masses at US: to biopsy or not to biopsy? Radiographics. 2013; 33:419–434. PMID: 23479705.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Imaging Features of the Mesenchymal Tumors of the Breast according to WHO Classification: A Pictorial Essay
- Breast lesions during pregnancy and lactation: a pictorial essay
- Sonographic Features of Palpable Breast and Axillary Lesions in Adult Male Patients: A Pictorial Essay
- Postoperative Imaging Findings of Colorectal Surgery: A Pictorial Essay
- Imaging Spectrum of Augmented Breast and Post-Mastectomy Reconstructed Breast with Common Complications: A Pictorial Essay
