Korean J Neurotrauma.
2018 Oct;14(2):155-158. 10.13004/kjnt.2018.14.2.155.
Tracheal Infection Resulting from High Endotracheal Tube Cuff Pressure in an Unconscious Patient with Brain Trauma
- Affiliations
-
- 1Department of Neurosurgery, Gyeongsang National University Hospital, Gyeongsang National University School of Medicine, Jinju, Korea. leeys1026@hanmail.net
- KMID: 2424331
- DOI: http://doi.org/10.13004/kjnt.2018.14.2.155
Abstract
- Deep neck infections (DNIs) are mainly caused by dental caries, tonsillitis, and pharyngitis; however, DNIs can also occur after head and neck trauma. A 79-year-old male patient underwent a craniectomy due to an acute subdural hematoma. The patient was unconscious and continued to have a fever, but no clear cause was found. On postoperative day 9, he suddenly showed redness and swelling on the anterior neck. Enhanced computed tomography of the pharynx revealed tracheal necrosis and an abscess in the surrounding area. An incision and drainage were performed and Enterobacter aerogenes and E. faecalis were identified. The infection was controlled after antibiotic treatment. High endotracheal tube cuff pressure was suspected as the cause of the tracheal infection. Although DNIs are difficult to predict in patients who cannot report their symptoms due to unconsciousness, prevention and rapid diagnosis are important, as DNIs have serious side effects.
MeSH Terms
Figure
-
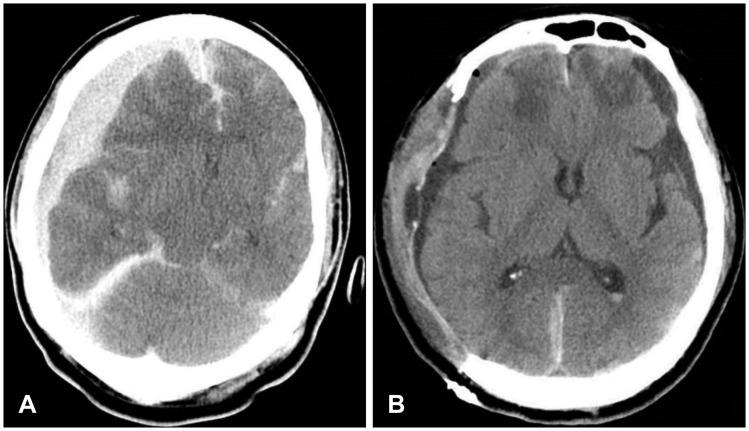
FIGURE 1 Preoperative and postoperative brain CT. (A) Preoperative brain CT scan shows increased right convexity subdural hematoma with midline shift to the left. (B) The CT scan from postoperative day 8 shows resolving hematoma and improved midline shifting.
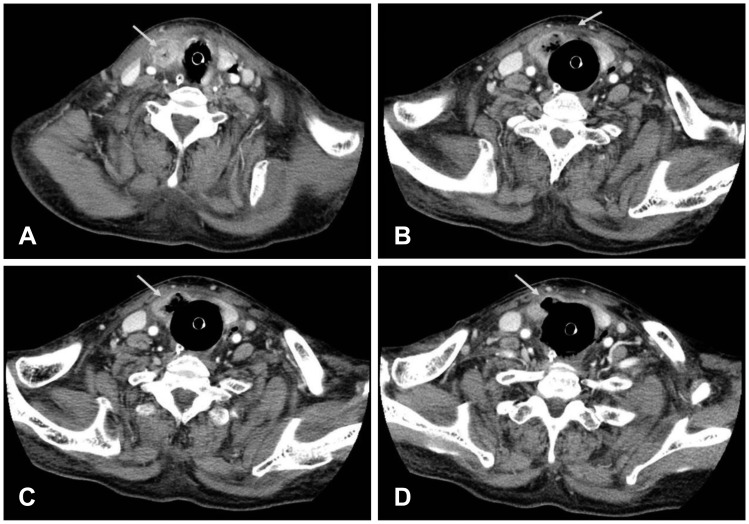
FIGURE 2 Contrast-enhanced neck CT scan. An over distension state of the upper (cervical) trachea and adjacent soft tissue with air bubbles around the trachea, the right thyroid gland, and both visceral spaces are shown (A and B). Severe infection and necrosis around the endotracheal tube cuff is revealed (C and D, white arrow).
Reference
-
1. Ballenger JJ, Snow JB. Otorhinolaryngology: head and neck surgery. ed 15th. Baltimore, MD: Williams & Wilkins;1996.2. Daramola OO, Flanagan CE, Maisel RH, Odland RM. Diagnosis and treatment of deep neck space abscesses. Otolaryngol Head Neck Surg. 2009; 141:123–130. PMID: 19559971.
Article3. Eggimann P, Pittet D. Infection control in the ICU. Chest. 2001; 120:2059–2093. PMID: 11742943.
Article4. Kinzer S, Pfeiffer J, Becker S, Ridder GJ. Severe deep neck space infections and mediastinitis of odontogenic origin: clinical relevance and implications for diagnosis and treatment. Acta Otolaryngol. 2009; 129:62–70. PMID: 18607917.
Article5. Levi ME, Eusterman VD. Oral infections and antibiotic therapy. Otolaryngol Clin North Am. 2011; 44:57–78. PMID: 21093623.
Article6. Orta DA, Cousar JE 3rd, Yergin BM, Olsen GN. Tracheal laceration with massive subcutaneous emphysema: a rare complication of endotracheal intubation. Thorax. 1979; 34:665–669. PMID: 515988.
Article7. Osborn TM, Assael LA, Bell RB. Deep space neck infection: principles of surgical management. Oral Maxillofac Surg Clin North Am. 2008; 20:353–365. PMID: 18603196.
Article8. Ryan M, Levy MM. Clinical review: fever in intensive care unit patients. Crit Care. 2003; 7:221–225. PMID: 12793871.9. Sethi DS, Stanley RE. Deep neck abscesses-changing trends. J Laryngol Otol. 1994; 108:138–143. PMID: 8163915.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Endotracheal Tube Cuff Volume and Pressure Changes in the Use of Nitrous Oxide
- Estimate the Cuff Inflation Volume to Maintain Safe Intracuff Pressure of an Endotracheal Tube
- Occurrence of Acquired Tracheoesophageal Fistula Due to Excess Endotracheal Tube Cuff Volumes: A Case Report
- Tracheal Puncture and Endotracheal Tube Cuff Perforation as a Complication of the Subclavian Vein Catheterization: A case report
- The Effects of Tidal Volume on Minimal Occlusion Pressure of Endotracheal Tube Cuff in Patients with Same Peak Inspiratory pressure
