Usefulness of transthoracic lung ultrasound for the diagnosis of mild pneumothorax
- Affiliations
-
- 1Institute of Animal Medicine, College of Veterinary Medicine, Gyeongsang National University, Jinju 52828, Korea. lhc@gnu.ac.kr
- 2College of Veterinary Medicine, Seoul National University, Seoul 08826, Korea.
- KMID: 2420935
- DOI: http://doi.org/10.4142/jvs.2018.19.5.660
Abstract
- The aim of the present study was to investigate the diagnostic accuracy of ultrasonography in the detection of mild pneumothorax using computed tomography (CT) in dogs. Nine adult healthy beagles were included in the study. A thoracic tube was inserted into pleural space at the left thoracic wall, and each dog underwent the examinations in the order of CT, lung ultrasonography, and radiography before the infusion of room air into the pleural space. Two, 3, and 5 mL/kg infusions of room air were sequentially introduced into the pleural space and CT, lung ultrasound, and radiography examinations were performed. Sonographic signs included A-lines, stratosphere, lung sliding, lung point, lung pulse, and reverse sliding signs. Radiographs were evaluated for the absence or presence of a pneumothorax. Lung ultrasound results were more accurate than radiography results for the detection of mild pneumothorax. The overall sensitivity of the sonographic reverse sliding sign was higher than that of other sonographic signs, and its specificity was 100% for detection of mild pneumothorax. Thus, the reverse sliding sign is useful when using lung ultrasonography for diagnosis of mild pneumothorax.
Keyword
MeSH Terms
Figure
-

Fig. 1 Diagnosis of pneumothorax by using computed tomography (CT). (A) Pneumothorax (arrows) of the cranial thorax on axial CT image. (B) Pneumothorax (arrows) of the caudal thorax on axial CT image.
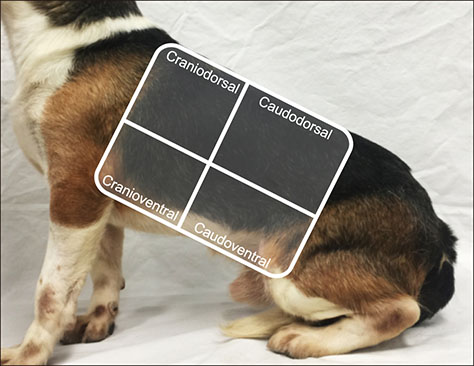
Fig. 2 Transthoracic lung ultrasound scan areas. Diagram illustrating location criteria used for dividing each dog's hemithorax into four quadrants, using the shoulder joint as the limit between the ventral and dorsal quadrants and the sixth intercostal space as the limit between the cranial and caudal quadrants.
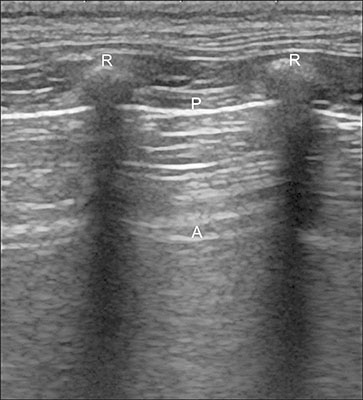
Fig. 3 Normal lung transthoracic ultrasound image. Horizontal A-lines are present in healthy dogs. R, rib; P, pleural surface; A, reverberation artefact of the pleural surface.
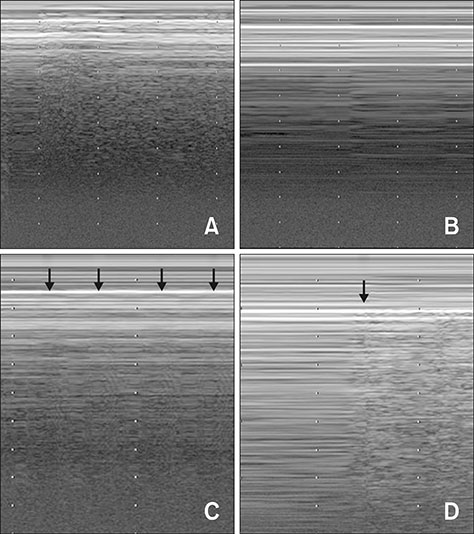
Fig. 4 The time-motion mode objectifies the lung slide (A), stratosphere (B), lung pulse (C), and lung point (D) signs. (A) Below the pleural line, lung sliding generates a homogeneous granular pattern. (B) Parallel horizontal lines above and below the pleural line, resemble a ‘barcode’ and indicates the absence of lung sliding. (C) Vertical movement of pleural lines synchronous to the cardiac rhythm (arrows). (D) The sudden inspiratory appearance of a granular pattern beneath the pleural line (arrow).
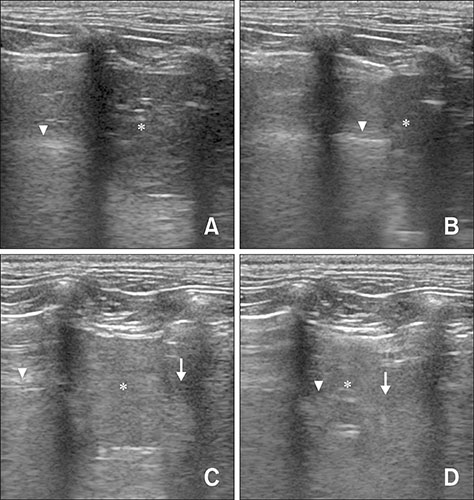
Fig. 5 The two-dimensional mode objectifies normal lung (A and B) and reverse sliding sign (C and D) in ultrasound images. (A) During expiration, horizontal A-lines (arrowhead) were present in healthy dogs. (B) During inspiration, A-lines showed lung sliding in the caudal direction (arrowhead). (C) During expiration, caudal lung lobe (arrowhead) was present. A minimal amount of trapped pleural air may remain in the caudodorsal thorax in the area of the adjacent rib (arrow). The trapped air visualized as A-line in this area. (D) During inspiration, the trapped pleural air escapes because of an increase in the size of the thoracic cavity. The half image under the transducer shows lung slide in the caudal direction (arrowhead), while the other half of the image shows the sliding sign in the opposite direction in the left caudodorsal thorax (arrow). Asterisks, left lateral hepatic lobe.
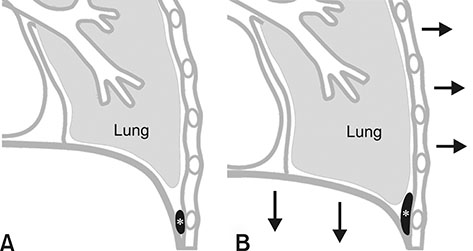
Fig. 6 A theoretical explanation of the reverse sliding sign. (A) During expiration, a minimal amount of pleural air (asterisk) may remain in the caudodorsal thorax in the area of the adjacent rib in sternal recumbency dogs. (B) During inspiration, trapped pleural air (asterisk) escapes because of increase in the size of the thoracic cavity; that is, the lung is inflated in the caudal direction during inspiration, while trapped air escapes in a direction opposite to that of lung sliding in the caudodorsal thorax.
Reference
-
1. Abdalla W, Elgendy M, Abdelaziz AA, Ammar MA. Lung ultrasound versus chest radiography for the diagnosis of pneumothorax in critically ill patients: a prospective, single-blind study. Saudi J Anaesth. 2016; 10:265–269.
Article2. Alrajab S, Youssef AM, Akkus NI, Caldito G. Pleural ultrasonography versus chest radiography for the diagnosis of pneumothorax: review of the literature and meta-analysis. Crit Care. 2013; 17:R208.
Article3. Barillari A, Kiuru S. Detection of spontaneous pneumothorax with chest ultrasound in the emergency department. Intern Emerg Med. 2010; 5:253–255.
Article4. Blaivas M, Lyon M, Duggal S. A prospective comparison of supine chest radiography and bedside ultrasound for the diagnosis of traumatic pneumothorax. Acad Emerg Med. 2005; 12:844–849.
Article5. Chiles C, Ravin CE. Radiographic recognition of pneumothorax in the intensive care unit. Crit Care Med. 1986; 14:677–680.
Article6. Chung MJ, Goo JM, Im JG, Cho JM, Cho SB, Kim SJ. Value of high-resolution ultrasound in detecting a pneumothorax. Eur Radiol. 2005; 15:930–935.
Article7. De Luca C, Valentino M, Rimondi MR, Branchini M, Baleni MC, Barozzi L. Use of chest sonography in acute-care radiology. J Ultrasound. 2008; 11:125–134.
Article8. Ding W, Shen Y, Yang J, He X, Zhang M. Diagnosis of pneumothorax by radiography and ultrasonography: a meta-analysis. Chest. 2011; 140:859–866.
Article9. Garofalo G, Busso M, Perotto F, De Pascale A, Fava C. Ultrasound diagnosis of pneumothorax. Radiol Med. 2006; 111:516–525.
Article10. Husain LF, Hagopian L, Wayman D, Baker WE, Carmody KA. Sonographic diagnosis of pneumothorax. J Emerg Trauma Shock. 2012; 5:76–81.
Article11. Johnson A. Emergency department diagnosis of pneumothorax using goal-directed ultrasound. Acad Emerg Med. 2009; 16:1379–1380.
Article12. Leigh-Smith S, Harris T. Tension pneumothorax: time for a re-think? Emerg Med J. 2005; 22:8–16.13. Lichtenstein D, Mezière G, Biderman P, Gepner A. The comet-tail artifact: an ultrasound sign ruling out pneumothorax. Intensive Care Med. 1999; 25:383–388.
Article14. Lichtenstein D, Mezière G, Biderman P, Gepner A. The “lung point”: an ultrasound sign specific to pneumothorax. Intensive Care Med. 2000; 26:1434–1440.
Article15. Lichtenstein DA. Ultrasound in the management of thoracic disease. Crit Care Med. 2007; 35:5 Suppl. S250–S261.
Article16. Lichtenstein DA, Menu Y. A bedside ultrasound sign ruling out pneumothorax in the critically ill: lung sliding. Chest. 1995; 108:1345–1348.
Article17. Lichtenstein DA, Mezière G, Lascols N, Biderman P, Courret JP, Gepner A, Goldstein I, Tenoudji-Cohen M. Ultrasound diagnosis of occult pneumothorax. Crit Care Med. 2005; 33:1231–1238.
Article18. Mathis G, Bitschnau R, Gehmacher O, Scheier M, Kopf A, Schwärzler B, Amann T, Doringer W, Hergan K. Chest ultrasound in diagnosis of pulmonary embolism in comparison to helical CT. Ultraschall Med. 1999; 20:54–59.
Article19. Piette E, Daoust R, Denault A. Basic concepts in the use of thoracic and lung ultrasound. Curr Opin Anaesthesiol. 2013; 26:20–30.
Article20. Reissig A, Heyne JP, Kroegel C. Sonography of lung and pleura in pulmonary embolism: sonomorphologic characterization and comparison with spiral CT scanning. Chest. 2001; 120:1977–1983.
Article21. Reißig A, Kroegel C. Accuracy of transthoracic sonography in excluding post-interventional pneumothorax and hydropneumothorax. Comparison to chest radiography. Eur J Radiol. 2005; 53:463–470.
Article22. Reissig A, Kroegel C. Transthoracic ultrasound of lung and pleura in the diagnosis of pulmonary embolism: a novel non-invasive bedside approach. Respiration. 2003; 70:441–452.
Article23. Sistrom CL, Reiheld CT, Gay SB, Wallace KK. Detection and estimation of the volume of pneumothorax using real-time sonography: efficacy determined by receiver operating characteristic analysis. AJR Am J Roentgenol. 1996; 166:317–321.
Article24. Soldati G, Testa A, Pignataro G, Portale G, Biasucci DG, Leone A, Silveri NG. The ultrasonographic deep sulcus sign in traumatic pneumothorax. Ultrasound Med Biol. 2006; 32:1157–1163.
Article25. Soldati G, Testa A, Sher S, Pignataro G, La Sala M, Silveri NG. Occult traumatic pneumothorax: diagnostic accuracy of lung ultrasonography in the emergency department. Chest. 2008; 133:204–211.26. Targhetta R, Bourgeois JM, Chavagneux R, Balmes P. Diagnosis of pneumothorax by ultrasound immediately after ultrasonically guided aspiration biopsy. Chest. 1992; 101:855–856.
Article27. Targhetta R, Bourgeois JM, Chavagneux R, Coste E, Amy D, Balmes P, Pourcelot L. Ultrasonic signs of pneumothorax: preliminary work. J Clin Ultrasound. 1993; 21:245–250.
Article28. Volpicelli G, Elbarbary M, Blaivas M, Lichtenstein DA, Mathis G, Kirkpatrick AW, Melniker L, Gargani L, Noble VE, Via G, Dean A, Tsung JW, Soldati G, Copetti R, Bouhemad B, Reissig A, Agricola E, Rouby JJ, Arbelot C, Liteplo A, Sargsyan A, Silva F, Hoppmann R, Breitkreutz R, Seibel A, Neri L, Storti E, Petrovic T. International Liaison Committee on Lung Ultrasound (ILC-LUS) for International Consensus Conference on Lung Ultrasound (ICC-LUS). International evidence-based recommendations for point-of-care lung ultrasound. Intensive Care Med. 2012; 38:577–591.
Article29. Warner BW, Bailey WW, Shipley RT. Value of computed tomography of the lung in the management of primary spontaneous pneumothorax. Am J Surg. 1991; 162:39–42.
Article30. Wernecke K. Ultrasound study of the pleura. Eur Radiol. 2000; 10:1515–1523.
Article31. Wernecke K, Galanski M, Peters PE, Hansen J. Pneumothorax: evaluation by ultrasound--preliminary results. J Thorac Imaging. 1987; 2:76–78.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ultrasonography-guided Transthoracic Cutting Biopsy of Pulmonary Lesion: Diagnostic Benefits and Safety
- Transthoracic needle biopsy for diagnosis of lung cancer
- Lung Ultrasound (in the Critically Ill) Superior to CT: the Example of Lung Sliding
- Transthoracic Needle Biopsy: How to Maximize Diagnostic Accuracy and Minimize Complications
- The Usefulness of Automated Biopsy Device for Lung Masses
