Korean J Gastroenterol.
2018 Sep;72(3):121-127. 10.4166/kjg.2018.72.3.121.
Clinical Response of Rifaximin Treatment in Patients with Abdominal Bloating
- Affiliations
-
- 1Department of Internal Medicine, Seoul National University Bundang Hospital, Seongnam, Korea. nayoungkim49@empas.com
- 2Department of Internal Medicine and Liver Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- KMID: 2420749
- DOI: http://doi.org/10.4166/kjg.2018.72.3.121
Abstract
- BACKGROUND/AIMS
Abdominal bloating is a troublesome complaint due to insufficient understanding of the pathophysiology. The aim of this study was to evaluate the efficacy of rifaximin in reducing bloating associated with functional gastrointestinal disorders (FGIDs).
METHODS
A total of 63 patients were treated with rifaximin for FGIDs with bloating or gas-related symptoms between 2007 and 2013 at Seoul National University Bundang Hospital. Rifaximin was administered at a dose between 800 mg/day and 1,200 mg/day for 5 to 14 days. The proportion of patients who had adequate relief of global FGID symptoms and FGID-related bloating was retrospectively assessed. The response was recorded when the symptoms were reduced by at least 50% at the follow-up after treatment cessation.
RESULTS
The mean age was 56.8±14.2 years; 49.2% were females. According to Rome III criteria, 20.6% (13/63) had irritable bowel syndrome (IBS) with constipation, 9.5% (6/63) had IBS with diarrhea, 4.8% (3/63) had mixed IBS, 23.8% (15/63) had functional dyspepsia, and 12.7% (8/63) had functional bloating. Of the 51 subjects who were followed-up, 30 (58.8%) had adequate relief of global FGID symptoms and 26 (51.0%) experienced improvement of abdominal bloating after rifaximin treatment. The proportion of female was slightly higher in non-response group than in the response group (60.0% vs. 34.6%, p=0.069). Otherwise, there was no difference between the two groups.
CONCLUSIONS
Despite the limitations of this retrospective study, our data confirms that rifaximin may be beneficial for abdominal bloating. Further prospective clinical trial with a larger cohort is needed.
MeSH Terms
Figure
-
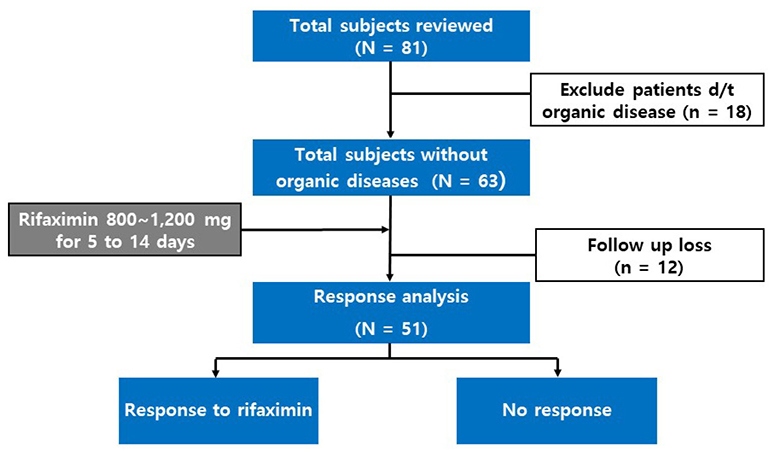
Fig. 1 Flow diagram of the study. After exclusion of 18 patients with organic disease, 51 patients with rifaximin treatment who had been followed-up were analyzed. d/t, due to.

Fig. 2 Diagnosis of enrolled patients. Functional bloating was defined as having recurrent bloating without meeting other functional gastrointestinal disorders, such as IBS or FD. FGID, functional gastrointestinal disorder; IBS-C, irritable bowel syndrome with constipation; IBS-D, irritable bowel syndrome with diarrhea; IBS-M, mixed type irritable bowel syndrome; FD, functional dyspepsia.
Cited by 1 articles
-
Duodenal Microbiome and Its Clinical Implications in Functional Dyspepsia
Sang Hoon Kim
Korean J Gastroenterol. 2022;79(3):91-98. doi: 10.4166/kjg.2022.027.
Reference
-
1. Issa B, Wafaei N, Whorwell PJ. Abdominal bloating and distension: what is the role of the microbiota. Dig Dis Sci. 2012; 57:4–8.
Article2. Seo AY, Kim N, Oh DH. Abdominal bloating: pathophysiology and treatment. J Neurogastroenterol Motil. 2013; 19:433–453.
Article3. Maxton DG, Morris JA, Whorwell PJ. Ranking of symptoms by patients with the irritable bowel syndrome. BMJ. 1989; 299:1138.
Article4. Collins SM, Denou E, Verdu EF, Bercik P. The putative role of the intestinal microbiota in the irritable bowel syndrome. Dig Liver Dis. 2009; 41:850–853.
Article5. Kassinen A, Krogius-Kurikka L, Mäkivuokko H, et al. The fecal microbiota of irritable bowel syndrome patients differs significantly from that of healthy subjects. Gastroenterology. 2007; 133:24–33.
Article6. King TS, Elia M, Hunter JO. Abnormal colonic fermentation in irritable bowel syndrome. Lancet. 1998; 352:1187–1189.
Article7. Balsari A, Ceccarelli A, Dubini F, Fesce E, Poli G. The fecal microbial population in the irritable bowel syndrome. Microbiologica. 1982; 5:185–194.8. Malinen E, Rinttilä T, Kajander K, et al. Analysis of the fecal microbiota of irritable bowel syndrome patients and healthy controls with real-time PCR. Am J Gastroenterol. 2005; 100:373–382.
Article9. Posserud I, Stotzer PO, Björnsson ES, Abrahamsson H, Simrén M. Small intestinal bacterial overgrowth in patients with irritable bowel syndrome. Gut. 2007; 56:802–808.
Article10. Marchese A, Salerno A, Pesce A, Debbia EA, Schito GC. In vitro activity of rifaximin, metronidazole and vancomycin against Clostridium difficile and the rate of selection of spontaneously resistant mutants against representative anaerobic and aerobic bacteria, including ammonia-producing species. Chemotherapy. 2000; 46:253–266.11. Spiller RC. Role of infection in irritable bowel syndrome. J Gastroenterol. 2007; 42:Suppl 17. 41–47.
Article12. Francis CY, Morris J, Whorwell PJ. The irritable bowel severity scoring system: a simple method of monitoring irritable bowel syndrome and its progress. Aliment Pharmacol Ther. 1997; 11:395–402.
Article13. Jiang X, Locke GR 3rd, Choung RS, Zinsmeister AR, Schleck C, Talley NJ. Prevalence and risk factors for abdominal bloating and visible distention: a population-based study. Gut. 2008; 57:756–763.
Article14. Ringel Y, Williams RE, Kalilani L, Cook SF. Prevalence, characteristics, and impact of bloating symptoms in patients with irritable bowel syndrome. Clin Gastroenterol Hepatol. 2009; 7:68–72. quiz 3.
Article15. Sandler RS, Stewart WF, Liberman JN, Ricci JA, Zorich NL. Abdominal pain, bloating, and diarrhea in the United States. Dig Dis Sci. 2000; 45:1166–1171.16. Houghton LA, Lea R, Agrawal A, Reilly B, Whorwell PJ. Relationship of abdominal bloating to distention in irritable bowel syndrome and effect of bowel habit. Gastroenterology. 2006; 131:1003–1010.
Article17. Lee BJ, Bak YT. Irritable bowel syndrome, gut microbiota and probiotics. J Neurogastroenterol Motil. 2011; 17:252–266.
Article18. Pimentel M, Park S, Mirocha J, Kane SV, Kong Y. The effect of a nonabsorbed oral antibiotic (rifaximin) on the symptoms of the irritable bowel syndrome: a randomized trial. Ann Intern Med. 2006; 145:557–563.19. Sharara AI, Aoun E, Abdul-Baki H, Mounzer R, Sidani S, ElHajj I. A randomized double-blind placebo-controlled trial of rifaximin in patients with abdominal bloating and flatulence. Am J Gastroenterol. 2006; 101:326–333.
Article20. Corazza GR, Ventrucci M, Strocchi A, et al. Treatment of small intestine bacterial overgrowth with rifaximin, a non-absorbable rifamycin. J Int Med Res. 1988; 16:312–316.
Article21. Di Stefano M, Malservisi S, Veneto G, Ferrieri A, Corazza GR. Rifaximin versus chlortetracycline in the short-term treatment of small intestinal bacterial overgrowth. Aliment Pharmacol Ther. 2000; 14:551–556.
Article22. Pimentel M, Lembo A, Chey WD, et al. Rifaximin therapy for patients with irritable bowel syndrome without constipation. N Engl J Med. 2011; 364:22–32.
Article23. Peralta S, Cottone C, Doveri T, Almasio PL, Craxi A. Small intestine bacterial overgrowth and irritable bowel syndrome-related symptoms: experience with rifaximin. World J Gastroenterol. 2009; 15:2628–2631.
Article24. Jolley J. High-dose rifaximin treatment alleviates global symptoms of irritable bowel syndrome. Clin Exp Gastroenterol. 2011; 4:43–48.
Article25. Yoshida M, Kinoshita Y, Watanabe M, Sugano K. JSGE clinical practice guidelines 2014: standards, methods, and process of developing the guidelines. J Gastroenterol. 2015; 50:4–10.
Article26. Lovell RM, Ford AC. Global prevalence of and risk factors for irritable bowel syndrome: a meta-analysis. Clin Gastroenterol Hepatol. 2012; 10:712–721.
Article27. Menees SB, Maneerattannaporn M, Kim HM, Chey WD. The efficacy and safety of rifaximin for the irritable bowel syndrome: a systematic review and meta-analysis. Am J Gastroenterol. 2012; 107:28–35. quiz 36.
Article28. Urita Y, Watanabe T, Takemoto I, et al. Intraluminal gas and gastrointestinal diseases. In : Yoshikawa T, Naito Y, editors. Gas biology research in clinical practice. 1st ed. Basel: S. Karger AG;2011. p. 6–14.29. O'Connor OJ, McSweeney SE, McWilliams S, et al. Role of radiologic imaging in irritable bowel syndrome: evidence-based review. Radiology. 2012; 262:485–494.30. Cash BD, Schoenfeld P, Chey WD. The utility of diagnostic tests in irritable bowel syndrome patients: a systematic review. Am J gastroenterol. 2002; 97:2812–2819.
Article31. Gans SL, Stoker J, Boermeester MA. Plain abdominal radiography in acute abdominal pain; past, present, and future. Int J Gen Med. 2012; 5:525–533.32. Chami TN, Schuster MM, Bohlman ME, Pulliam TJ, Kamal N, Whitehead WE. A simple radiologic method to estimate the quantity of bowel gas. Am J Gastroenterol. 1991; 86:599–602.33. Koide A, Yamaguchi T, Odaka T, et al. Quantitative analysis of bowel gas using plain abdominal radiograph in patients with irritable bowel syndrome. Am J Gastroenterol. 2000; 95:1735–1741.
Article34. Morken MH, Berstad AE, Nysaeter G, Berstad A. Intestinal gas in plain abdominal radiographs does not correlate with symptoms after lactulose challenge. Eur J Gastroenterol Hepatol. 2007; 19:589–593.
Article35. Tana C, Umesaki Y, Imaoka A, Handa T, Kanazawa M, Fukudo S. Altered profiles of intestinal microbiota and organic acids may be the origin of symptoms in irritable bowel syndrome. Neurogastroenterol Motil. 2010; 22:512–519. e114–e115.
Article36. Pimentel M, Morales W, Chua K, et al. Effects of rifaximin treatment and retreatment in nonconstipated IBS subjects. Dig Dis Sci. 2011; 56:2067–2072.
Article37. Lembo A, Pimentel M, Rao SS, et al. Repeat treatment with rifaximin is safe and effective in patients with diarrhea-predominant irritable bowel syndrome. Gastroenterology. 2016; 151:1113–1121.
Article38. DuPont HL. Review article: the antimicrobial effects of rifaximin on the gut microbiota. Aliment Pharmacol Ther. 2016; 43:Suppl 1. 3–10.
Article39. Soldi S, Vasileiadis S, Uggeri F, et al. Modulation of the gut microbiota composition by rifaximin in non-constipated irritable bowel syndrome patients: a molecular approach. Clin Exp Gastroenterol. 2015; 8:309–325.
Article40. Xu D, Gao J, Gillilland M 3rd, et al. Rifaximin alters intestinal bacteria and prevents stress-induced gut inflammation and visceral hyperalgesia in rats. Gastroenterology. 2014; 146:484–496.e4.
Article41. Tan VP, Liu KS, Lam FY, Hung IF, Yuen MF, Leung WK. Randomised clinical trial: rifaximin versus placebo for the treatment of functional dyspepsia. Aliment Pharmacol Ther. 2017; 45:767–776.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Abdominal Bloating: Pathophysiology and Treatment
- Effect of Trimebutine and Rifaximin on Breath Hydrogen and Methane by Glucose Breath Test in Patients With Functional Bloating: A Randomized Double-blind Clinical Trial
- Diagnosis and Treatment of Functional Bloating
- Efficacy and Safety of Short-term Administration of Rifaximin in the Treatment of Hepatic Encephalopathy
- Effects of Korean Hand Acupressure on Pain and Abdominal Bloating of Patients Receiving Laparoscopic Hysterectomy
