A novel classification of anterior alveolar arch forms and alveolar bone thickness: A cone-beam computed tomography study
- Affiliations
-
- 1Esthetic Restorative and Implant Dentistry Program, Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand. atiphan.p@chula.ac.th
- 2Department of Oral and Maxillofacial Surgery, Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand.
- KMID: 2420547
- DOI: http://doi.org/10.5624/isd.2018.48.3.191
Abstract
- PURPOSE
This study classified alveolar arch forms and evaluated differences in alveolar bone thickness among arch forms in the anterior esthetic region using cone-beam computed tomography (CBCT) images.
MATERIALS AND METHODS
Axial views of 113 CBCT images were assessed at the level of 3 mm below the cementoenamel junction (CEJ) of the right and left canines. The root center points of teeth in the anterior esthetic region were used as reference points. Arch forms were classified according to their transverse dimensions and the intercanine width-to-depth ratio. The buccolingual alveolar bone thickness of each tooth was measured at 3 mm below the CEJ and at the mid-root level. Differences in the mean thicknesses among arch forms were analyzed.
RESULTS
Anterior maxillary arches could be classified as long narrow, short medium, long medium, and long wide arches. Significant differences in buccolingual alveolar bone thickness among the arch groups were found at both levels. The long wide arches presented the greatest bone thickness, followed by the long medium arches, while the long narrow and short medium arches were the thinnest.
CONCLUSION
Arch forms were classified as long narrow, short medium, long medium, and long wide. The buccolingual alveolar bone thickness exhibited significant differences among the arch forms.
Figure
-

Fig. 1 Example of a maxillary alveolar arch, where a and a′ are the root center points of central incisors. The aa′ line is the line that links the a and a′ points. b and b′ are the root center points of the canines. The line that links the b and b′ points (bb′ line) is the intercanine width. c and c′ are the root center points of the first premolars. The line between the c and c′ points (cc′ line) is the interpremolar width. am is the midpoint of the aa′ line. The bm point is the endpoint of the perpendicular line originating from am and extending to the bb′ line. The ambm line is the intercanine depth. The cm point is the endpoint of the perpendicular line originating from am to the cc′ line. The amcm line is the interpremolar depth.
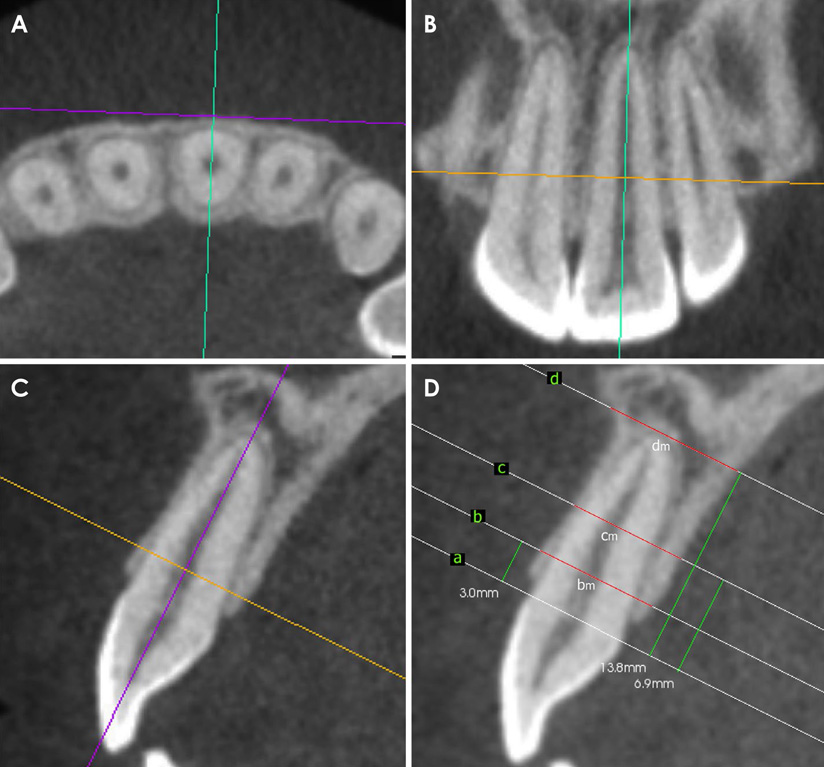
Fig. 2 A. A cone-beam computed tomographic (CBCT) image in the axial plane sliced perpendicular to the labial or buccal contour of the alveolar bone of the left central incisor. B. A CBCT image in the coronal plane sliced parallel to the root axis of the left central incisor. C. A CBCT image in the sagittal plane sliced parallel to the root axis of the left central incisor. D. The measurement of buccolingual alveolar bone thickness: the a level is at the cementoenamel junction (CEJ) level of the left central incisor, the b level is 3 mm below the CEJ, the c level is the level of the mid-root, and the d level is the level of the root apex. Alveolar buccolingual thickness was measured perpendicular to the long axis at 3 mm below the CEJ (B) and at the mid-root (C). The distance bm is the buccolingual alveolar bone thickness at 3 mm below the CEJ, and cm is the buccolingual alveolar bone thickness at the level of the mid-root.
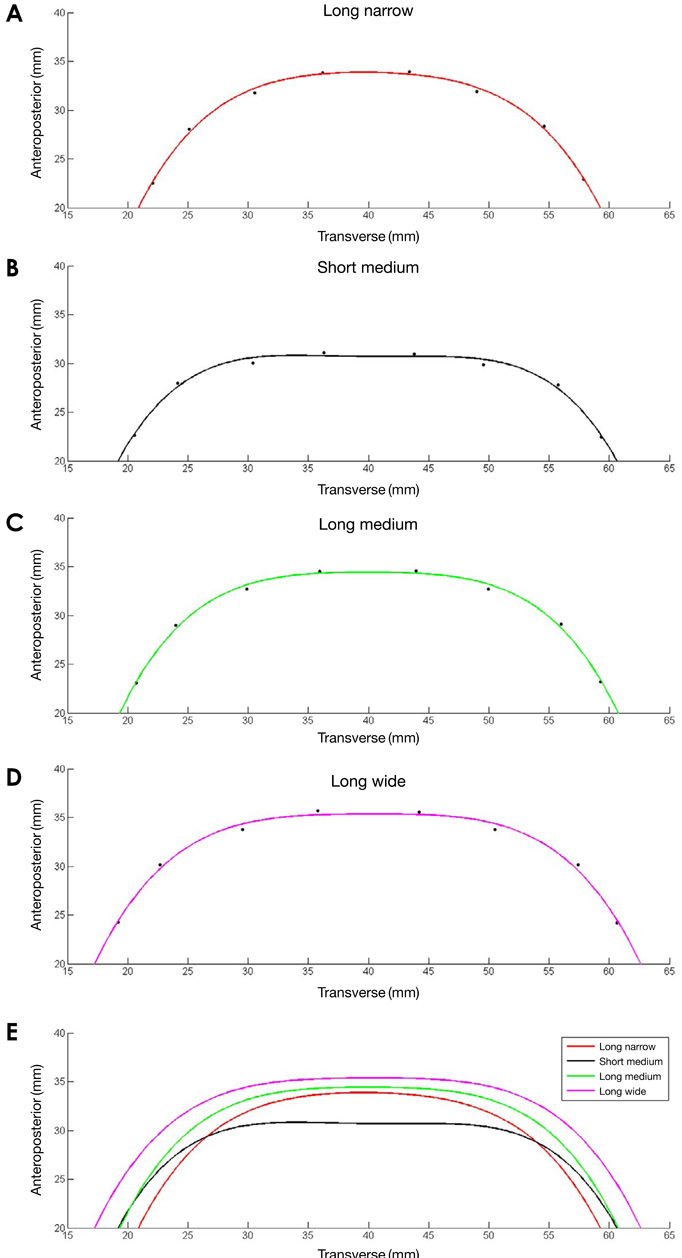
Fig. 3 The best-fit curves plotted using the mean coordinates of the subjects in each cluster. A. Long narrow arch form. B. Short medium arch form. C. Long medium arch form. D. Long wide arch form. E. Comparison of the best-fit curve among the clusters.
Cited by 1 articles
-
Cone-beam computed tomographic analysis of the alveolar ridge profile and virtual implant placement for the anterior maxilla
Hyun-Chang Lim, Do-Uk Kang, Hyehyeon Baek, Ji-Youn Hong, Seung-Yun Shin, Jong-Hyuk Chung, Yeek Herr, Seung-Il Shin
J Periodontal Implant Sci. 2019;49(5):299-309. doi: 10.5051/jpis.2019.49.5.299.
Reference
-
1. Araújo MG, Lindhe J. Dimensional ridge alterations following tooth extraction. An experimental study in the dog. J Clin Periodontol. 2005; 32:212–218.
Article2. Misch CE. Stress treatment theorem for implant dentistry. In : Misch CE, editor. Contemporary implant dentistry. 3rd ed. St. Louis: Mosby;2008. p. 68–91.3. Misch CE. Treatment plans related to key implant positions and implant numbers. In : Misch CE, editor. Contemporary implant dentistry. 3rd ed. St. Louis: Mosby;2008. p. 147–159.4. Sagat G, Yalcin S, Gultekin BA, Mijiritsky E. Influence of arch shape and implant position on stress distribution around implants supporting fixed full-arch prosthesis in edentulous maxilla. Implant Dent. 2010; 19:498–508.
Article5. Braun S, Hnat WP, Fender DE, Legan HL. The form of the human dental arch. Angle Orthod. 1998; 68:29–36.6. Currier JH. A computerized geometric analysis of human dental arch form. Am J Orthod. 1969; 56:164–179.
Article7. Noroozi H, Nik TH, Saeeda R. The dental arch form revisited. Angle Orthod. 2001; 71:386–389.8. Lee SJ, Lee S, Lim J, Park HJ, Wheeler TT. Method to classify dental arch forms. Am J Orthod Dentofacial Orthop. 2011; 140:87–96.
Article9. Bayome M, Han SH, Choi JH, Kim SH, Baek SH, Kim DJ, et al. New clinical classification of dental arch form using facial axis points derived from three-dimensional models. Aust Orthod J. 2011; 27:117–124.10. Ronay V, Miner RM, Will LA, Arai K. Mandibular arch form: the relationship between dental and basal anatomy. Am J Orthod Dentofacial Orthop. 2008; 134:430–438.
Article11. Braut V, Bornstein MM, Belser U, Buser D. Thickness of the anterior maxillary facial bone wall - a retrospective radiographic study using cone beam computed tomography. Int J Periodontics Restorative Dent. 2011; 31:125–131.12. Ghassemian M, Nowzari H, Lajolo C, Verdugo F, Pirronti T, D'Addona A. The thickness of facial alveolar bone overlying healthy maxillary anterior teeth. J Periodontol. 2012; 83:187–197.
Article13. Jin SH, Park JB, Kim N, Park S, Kim KJ, Kim Y, et al. The thickness of alveolar bone at the maxillary canine and premolar teeth in normal occlusion. J Periodontal Implant Sci. 2012; 42:173–178.
Article14. Lee SL, Kim HJ, Son MK, Chung CH. Anthropometric analysis of maxillary anterior buccal bone of Korean adults using cone-beam CT. J Adv Prosthodont. 2010; 2:92–96.
Article15. Naitoh M, Hayashi H, Tsukamoto N, Ariji E. Labial bone assessment surrounding dental implant using cone-beam computed tomography: an in vitro study. Clin Oral Implants Res. 2012; 23:970–974.
Article16. Vera C, De Kok IJ, Reinhold D, Limpiphipatanakorn P, Yap AK, Tyndall D, et al. Evaluation of buccal alveolar bone dimension of maxillary anterior and premolar teeth: a cone beam computed tomography investigation. Int J Oral Maxillofac Implants. 2012; 27:1514–1519.17. Januario AL, Duarte WR, Barriviera M, Mesti JC, Araujo MG, Lindhe J. Dimension of the facial bone wall in the anterior maxilla: a cone-beam computed tomography study. Clin Oral Implants Res. 2011; 22:1168–1171.18. Suk KE, Park JH, Bayome M, Nam YO, Sameshima GT, Kook YA. Comparison between dental and basal arch forms in normal occlusion and Class III malocclusions utilizing cone-beam computed tomography. Korean J Orthod. 2013; 43:15–22.
Article19. Bayome M, Park JH, Han SH, Baek SH, Sameshima GT, Kook YA. Evaluation of dental and basal arch forms using cone-beam CT and 3D virtual models of normal occlusion. Aust Orthod J. 2013; 29:43–51.20. Buser D, Martin W, Belser UC. Optimizing esthetics for implant restorations in the anterior maxilla: anatomic and surgical considerations. Int J Oral Maxillofac Implants. 2004; 19:Suppl. 43–61.21. Grunder U, Gracis S, Capelli M. Influence of the 3-D bone-to-implant relationship on esthetics. Int J Periodontics Restorative Dent. 2005; 25:113–119.22. Darby I, Chen ST, Buser D. Ridge preservation techniques for implant therapy. Int J Oral Maxillofac Implants. 2009; 24:Suppl. 260–271.23. von Arx T, Buser D. Horizontal ridge augmentation using autogenous block grafts and the guided bone regeneration technique with collagen membranes: a clinical study with 42 patients. Clin Oral Implants Res. 2006; 17:359–366.
Article24. Ferrario VF, Sforza C, Miani A Jr, Tartaglia G. Mathematical definition of the shape of dental arches in human permanent healthy dentitions. Eur J Orthod. 1994; 16:287–294.
Article25. Park KH, Bayome M, Park JH, Lee JW, Baek SH, Kook YA. New classification of lingual arch form in normal occlusion using three dimensional virtual models. Korean J Orthod. 2015; 45:74–81.
Article26. Saadoun AP. The key to peri-implant esthetics: hard- and soft-tissue management. Dent Implantol Update. 1997; 8:41–46.27. Palacci P, Nowzari H. Soft tissue enhancement around dental implants. Periodontol 2000. 2008; 47:113–132.
Article28. Chu SJ, Tan JH, Stappert CF, Tarnow DP. Gingival zenith positions and levels of the maxillary anterior dentition. J Esthet Restor Dent. 2009; 21:113–120.
Article29. Duran I, Yilmaz B, Tatar N, Ural C, Guler AU. Determining the localization of premolar zenith positions according to the gingival line. Niger J Clin Pract. 2015; 18:273–275.
Article30. Preti G, Pera P, Bassi F. Prediction of the shape and size of the maxillary anterior arch in edentulous patients. J Oral Rehabil. 1986; 13:115–125.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Influence of the anterior arch shape and root position on root angulation in the maxillary esthetic area
- Associations among the anterior maxillary dental arch form, alveolar bone thickness, and the sagittal root position of the maxillary central incisors in relation to immediate implant placement: A cone-beam computed tomography analysis
- Evaluation of changes in the maxillary alveolar bone after incisor intrusion
- Three-dimensional evaluation of maxillary anterior alveolar bone for optimal placement of miniscrew implants
- Alveolar bone thickness around maxillary central incisors of different inclination assessed with cone-beam computed tomography
