Obstet Gynecol Sci.
2018 Jan;61(1):135-141. 10.5468/ogs.2018.61.1.135.
Is robot-assisted laparoscopic myomectomy limited in multiple myomas?: a feasibility for ten or more myomas
- Affiliations
-
- 1Seoul St. Mary's Fibroid Center, Department of Obstetrics and Gynecology, College of Medicine, The Catholic University of Korea, Seoul, Korea. mrkim@catholic.ac.kr
- KMID: 2420162
- DOI: http://doi.org/10.5468/ogs.2018.61.1.135
Abstract
OBJECTIVE
To evaluate the feasibility of robot-assisted laparoscopic myomectomy in multiple myomas over 10.
METHODS
A retrospective study was conducted for 662 patients who underwent robot-assisted laparoscopic myomectomy and open myomectomy by a single operator in a tertiary university hospital.
RESULTS
A total of 30 women underwent removal of 10 or more uterine myomas by robotics and 13 patients were selected for this study. The average number of myomas removed was 13.7 (range 10-20). The maximum diameter of the myomas was 6.8 cm (range 5.0-10.0 cm). The sum of the diameters of each myoma was 34.7 cm (range 20.0-54.5 cm) and the mass of resected myomas for each case was 229.1 g (range 106.8-437.9 g). In no case was the robotic procedure converted into conventional laparoscopy or laparotomy, and all patients recovered without any major complications. In comparison with 13 cases of open myomectomy during the same period, robotic surgery took longer time than open surgery (360.5 vs. 183.8 minutes; P=0.001) but had shorter postoperative hospital days after surgery (mean 2.5 vs. 3.5 days; P=0.003).
CONCLUSION
Robot-assisted laparoscopic myomectomy could be an alternative to laparotomic myomectomy for numerous myomas over 10 in number.
Keyword
MeSH Terms
Figure
-
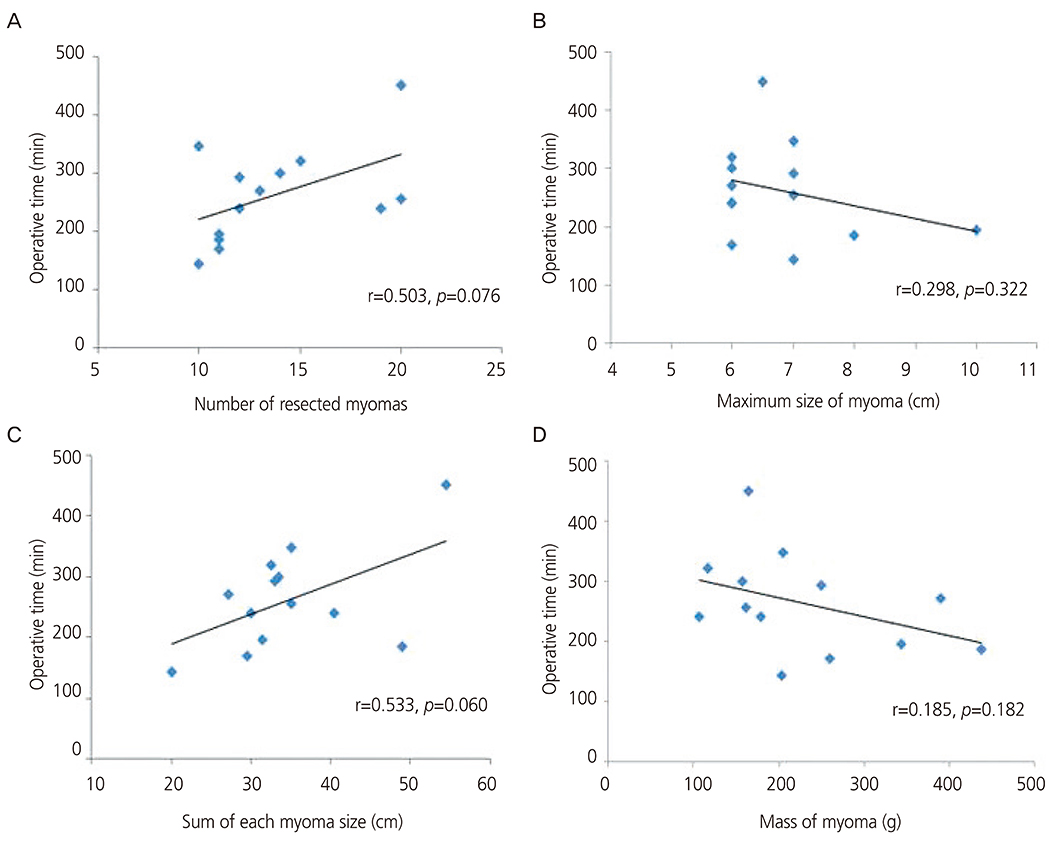
Fig. 1 The relations between the operative time and the characteristics of the removed myomas. (A) The number of resected myomas, (B) the maximum diameter of the myomas, (C) the sum of the diameters, and (D) the mass of resected myomas were not significantly correlated with the operative time.
Cited by 1 articles
-
Clinical experience of robotic myomectomy for fertility preservation using preoperative magnetic resonance imaging predictor
So Yun Park, Juhui Kim, Kyungah Jeong, Sung Il Jung, Young Min Hur, Eun Hye Cho, Hye-Sung Moon, Hye Won Chung
Obstet Gynecol Sci. 2020;63(6):726-734. doi: 10.5468/ogs.20145.
Reference
-
1. Practice Committee of the American Society for Reproductive Medicine. Myomas and reproductive function. Fertil Steril. 2004; 82:Suppl 1. S111–S116.2. Somigliana E, Vercellini P, Daguati R, Pasin R, De Giorgi O, Crosignani PG. Fibroids and female reproduction: a critical analysis of the evidence. Hum Reprod Update. 2007; 13:465–476.
Article3. Pritts EA, Parker WH, Olive DL. Fibroids and infertility: an updated systematic review of the evidence. Fertil Steril. 2009; 91:1215–1223.
Article4. Seracchioli R, Rossi S, Govoni F, Rossi E, Venturoli S, Bulletti C, et al. Fertility and obstetric outcome after laparoscopic myomectomy of large myomata: a randomized comparison with abdominal myomectomy. Hum Reprod. 2000; 15:2663–2668.
Article5. Mais V, Ajossa S, Guerriero S, Mascia M, Solla E, Melis GB. Laparoscopic versus abdominal myomectomy: a prospective, randomized trial to evaluate benefits in early outcome. Am J Obstet Gynecol. 1996; 174:654–658.
Article6. Bedient CE, Magrina JF, Noble BN, Kho RM. Comparison of robotic and laparoscopic myomectomy. Am J Obstet Gynecol. 2009; 201:566.e1–566.e5.
Article7. Hurst BS, Matthews ML, Marshburn PB. Laparoscopic myomectomy for symptomatic uterine myomas. Fertil Steril. 2005; 83:1–23.
Article8. Ascher-Walsh CJ, Capes TL. Robot-assisted laparoscopic myomectomy is an improvement over laparotomy in women with a limited number of myomas. J Minim Invasive Gynecol. 2010; 17:306–310.
Article9. Chiou HY, Chiu LH, Chen CH, Yen YK, Chang CW, Liu WM. Comparing robotic surgery with laparoscopy and laparotomy for endometrial cancer management: a cohort study. Int J Surg. 2015; 13:17–22.
Article10. Dubuisson J, Botchorishvili R, Perrette S, Bourdel N, Jardon K, Rabischong B, et al. Incidence of intraabdominal adhesions in a continuous series of 1000 laparoscopic procedures. Am J Obstet Gynecol. 2010; 203:111.e1–111.e3.
Article11. Advincula AP, Xu X, Goudeau S 4th, Ransom SB. Robot-assisted laparoscopic myomectomy versus abdominal myomectomy: a comparison of short-term surgical outcomes and immediate costs. J Minim Invasive Gynecol. 2007; 14:698–705.
Article12. Parker WH, Einarsson J, Istre O, Dubuisson JB. Risk factors for uterine rupture after laparoscopic myomectomy. J Minim Invasive Gynecol. 2010; 17:551–554.
Article13. Nezhat C, Lavie O, Hsu S, Watson J, Barnett O, Lemyre M. Robotic-assisted laparoscopic myomectomy compared with standard laparoscopic myomectomy--a retrospective matched control study. Fertil Steril. 2009; 91:556–559.
Article14. Ten Broek RP, Kok-Krant N, Bakkum EA, Bleichrodt RP, van Goor H. Different surgical techniques to reduce post-operative adhesion formation: a systematic review and meta-analysis. Hum Reprod Update. 2013; 19:12–25.
Article15. Advincula AP, Song A. The role of robotic surgery in gynecology. Curr Opin Obstet Gynecol. 2007; 19:331–336.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Surgical outcomes for robot-assisted laparoscopic myomectomy compared with laparoscopic myomectomy
- Robot-Assisted Laparoscopic Myomectomy versus Abdominal Myomectomy for Large Myomas Sized over 10 cm or Weighing 250 g
- Lack of Haptic Feedback Is Replaced by More Developed Visual Sense during Robotic Myomectomy
- The feasibility of robot-assisted laparoscopic myomectomy: Compared with standard laparoscopic and abdominal myomectomy
- Fertility Issues in Patients with Myoma
