Comparison of the Results between Conservative and Operative Treatments for Pyogenic Spondylitis
- Affiliations
-
- 1Department of Orthopaedic Surgery, Soonchunhyang University Cheonan Hospital, Soonchunhyang University College of Medicine, Cheonan, Korea. kwj9383@hanmail.net
- KMID: 2419469
- DOI: http://doi.org/10.4055/jkoa.2018.53.4.332
Abstract
- PURPOSE
With advancements in antibiotics, the ability to treat pyogenic spondylitis is increasing. This study aimed to compare and analyze the outcomes between conservative and operative treatments.
MATERIALS AND METHODS
Sixty patients (28 males and 32 females) with pyogenic spondylitis, who were hospitalized and treated between February 2008 and June 2016, were enrolled. Patients were divided according to the following: type of treatment - conservative or operative treatment, method of surgery, radiographic parameters, location of the affected spine. Clinical parameters as durations of hospital stay, intravenous antibiotics use, normalization in laboratory findings, and residual symptoms were analyzed. For statistical evaluation, independent-sample t-test, Mann-Whitney U-test, Pearson's chi-square test, one-way ANOVA, and Spearman correlation analysis were performed retrospectively.
RESULTS
There was no significant difference in the duration of hospital stay, intravenous antibiotics use, normalization in laboratory findings, and residual symptoms between the conservative and operative treatment groups.
CONCLUSION
In treating pyogenic spondylitis, conservative treatment can be considered as the first choice, and operative treatment can be chosen in refractory cases.
MeSH Terms
Figure
-

Figure 1 A 77-year-old female developed T8–9 pyogenic spondylitis. (A) Initial thoracic spine anteroposterior (AP) and lateral radiographs show severe disc space narrowing and end-plate destruction on T8–9. (B) Magnetic resonance imaging shows low-density signal changes in T8 and T9 in a T1-weighted image and enhancement in T8 and T9 along with inflammatory changes in the paraspinal soft tissue and epidural abscess. (C) Immediate postoperative thoracic spine AP and lateral radiographs. (D) Thoracic spine AP and lateral radiographs taken 12 months after operative treatment show no significant changes compared with the postoperative radiographs.
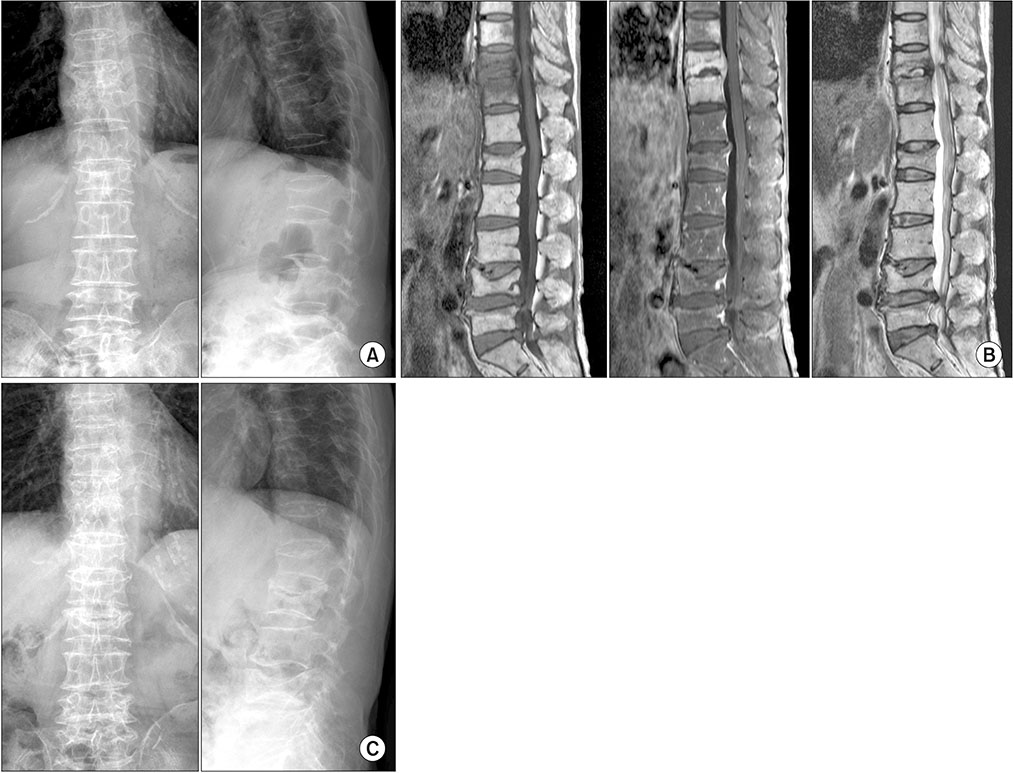
Figure 2 A 62-year-old female developed T10–11 pyogenic spondylitis. (A) Initial thoracolumbar spine anteroposterior (AP) and lateral radiographs show moderate disc space narrowing and end-plate destruction on T10–11. (B) Magnetic resonance imaging shows low-density signal changes in T10 and T11 in a T1-weighted image and enhancement in T10 and T11 with anterior epidural inflammatory thickening. (C) Thoracolumbar spine AP and lateral radiographs taken 12 months after conservative treatment demonstrate no significant changes compared with the initial radiographs.
Reference
-
1. Thelander U, Larsson S. Quantitation of C-reactive protein levels and erythrocyte sedimentation rate after spinal surgery. Spine (Phila Pa 1976). 1992; 17:400–404.
Article2. Butler JS, Shelly MJ, Timlin M, Powderly WG, O'Byrne JM. Nontuberculous pyogenic spinal infection in adults: a 12-year experience from a tertiary referral center. Spine (Phila Pa 1976). 2006; 31:2695–2700.3. Griffiths HE, Jones DM. Pyogenic infection of the spine. A review of twenty-eight cases. J Bone Joint Surg Br. 1971; 53:383–391.4. Lehovsky J. Pyogenic vertebral osteomyelitis/disc infection. Baillieres Best Pract Res Clin Rheumatol. 1999; 13:59–75.
Article5. Maiuri F, Iaconetta G, Gallicchio B, Manto A, Briganti F. Spondylodiscitis. Clinical and magnetic resonance diagnosis. Spine (Phila Pa 1976). 1997; 22:1741–1746.6. Bettini N, Girardo M, Dema E, Cervellati S. Evaluation of conservative treatment of non specific spondylodiscitis. Eur Spine J. 2009; 18:Suppl 1. 143–150.
Article7. Okada Y, Miyamoto H, Uno K, Sumi M. Clinical and radiological outcome of surgery for pyogenic and tuberculous spondylitis: comparisons of surgical techniques and disease types. J Neurosurg Spine. 2009; 11:620–627.
Article8. Kang DG, Kim DH, Park HB, Mun JU, Jeong ST. Conservative treatment of pyogenic spondylitis in the elderly. J Korean Soc Spine Surg. 2017; 24:7–15.
Article9. Valancius K, Hansen ES, Høy K, Helmig P, Niedermann B, Bünger C. Failure modes in conservative and surgical management of infectious spondylodiscitis. Eur Spine J. 2013; 22:1837–1844.
Article10. Chidiac C, Bru J, Choutet P, et al. Spondylodiscites infectieuses primitives, et secondaires à un geste intra-discal, sans mise en place de matériel. Méd Mal Infect. 2007; 37:554–572.11. Rutges JP, Kempen DH, van Dijk M, Oner FC. Outcome of conservative and surgical treatment of pyogenic spondylodiscitis: a systematic literature review. Eur Spine J. 2016; 25:983–999.
Article12. Yee DK, Samartzis D, Wong YW, Luk KD, Cheung KM. Infective spondylitis in Southern Chinese: a descriptive and comparative study of ninety-one cases. Spine (Phila Pa 1976). 2010; 35:635–641.13. Emery SE, Chan DP, Woodward HR. Treatment of hematogenous pyogenic vertebral osteomyelitis with anterior debridement and primary bone grafting. Spine (Phila Pa 1976). 1989; 14:284–291.14. McHenry MC, Easley KA, Locker GA. Vertebral osteomyelitis: long-term outcome for 253 patients from 7 Cleveland-area hospitals. Clin Infect Dis. 2002; 34:1342–1350.
Article15. Carragee EJ. Pyogenic vertebral osteomyelitis. J Bone Joint Surg Am. 1997; 79:874–880.
Article16. Dagirmanjian A, Schils J, McHenry MC. MR imaging of spinal infections. Magn Reson Imaging Clin N Am. 1999; 7:525–538.
Article17. Sharif HS. Role of MR imaging in the management of spinal infections. AJR Am J Roentgenol. 1992; 158:1333–1345.
Article18. Yoshimoto M, Takebayashi T, Kawaguchi S, et al. Pyogenic spondylitis in the elderly: a report from Japan with the most aging society. Eur Spine J. 2011; 20:649–654.
Article19. Digby JM, Kersley JB. Pyogenic non-tuberculous spinal infection: an analysis of thirty cases. J Bone Joint Surg Br. 1979; 61:47–55.
Article20. Suess O, Weise L, Brock M, Kombos T. Debridement and spinal instrumentation as a single-stage procedure in bacterial spondylitis/spondylodiscitis. Zentralbl Neurochir. 2007; 68:123–132.
Article21. Hadjipavlou AG, Katonis PK, Gaitanis IN, Muffoletto AJ, Tzermiadianos MN, Crow W. Percutaneous transpedicular discectomy and drainage in pyogenic spondylodiscitis. Eur Spine J. 2004; 13:707–713.
Article22. Torda AJ, Gottlieb T, Bradbury R. Pyogenic vertebral osteomyelitis: analysis of 20 cases and review. Clin Infect Dis. 1995; 20:320–328.
Article23. Kim YM, Won CH, Seo JB, Choi ES, Lee HS, Um SM. Pyogenic L4-5 spondylitis managed with percutaneous drainage followed by posterior lumbar interbody fusion: a case report. J Korean Soc Spine Surg. 2001; 8:513–519.24. Levi AD, Dickman CA, Sonntag VK. Management of postoperative infections after spinal instrumentation. J Neurosurg. 1997; 86:975–980.
Article25. Nene A, Bhojraj S. Results of nonsurgical treatment of thoracic spinal tuberculosis in adults. Spine J. 2005; 5:79–84.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Comparison of Pyogenic Spondylitis and Tuberculous Spondylitis
- Comparison of Pyogenic and Tuberculous Spondylitis
- 3 Cases of Pyogenic spondylitis
- Streptococcus Spondylitis Concomitant Infectious Endocarditis: A Case Report
- Preoperative Gadolinium-enhanced Magnetic Resonance Images on Infectious Spondylitis
