Continuing five or more locoregional therapies before living donor salvage liver transplantation for hepatocellular carcinoma is related to poor recurrence-free survival
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. yjongman21@gmail.com
- KMID: 2419446
- DOI: http://doi.org/10.4174/astr.2018.95.3.152
Abstract
- PURPOSE
This study was designed to analyze factors related to the success of salvage liver transplantation (SLT) in hepatocellular carcinoma (HCC). While liver resection (LR) is considered the best locoregional therapy in HCC, there is a high recurrence rate. SLT may be the best treatment option when feasible.
METHODS
Patients who underwent living donor SLT for recurrent HCC after LR from November 1996 to May 2017 were included. Patient demographic data, clinical and pathologic characteristics, operative data, hospital course, and follow-up data regarding initial LR, locoregional therapy after recurrence and SLT were reviewed. Prognostic factors for recurrence were analyzed using Cox proportional hazard ratio.
RESULTS
Eighty-five of 123 SLT patients were included. Patients who had five or more locoregional therapies prior to SLT (hazard ratio [HR], 3.74; 95% confidence interval [CI], 1.45-9.64, P = 0.006), hepatitis B (HR, 9.20; 95% CI, 1.13-74.89; P = 0.04), outside Milan criteria at the time of SLT (HR, 2.66, 95% CI, 1.26-5.63; P = 0.011) and an alpha-fetoprotein level above 1,000 ng/mL at the time of recurrence after initial LR (HR, 6.48; 95% CI, 1.83-22.92; P = 0.004) and at the time of transplantation (HR, 3.43; 95% CI, 1.26-5.63; P = 0.011) were related to significant risk of recurrence.
CONCLUSION
Continuing five or more locoregional therapies for recurrent HCC after LR is related to poor recurrence-free survival after SLT.
MeSH Terms
Figure
-

Fig. 1 A total of 85 patients were included in the study after excluding patients who underwent salvage liver transplantation due to liver failure (n = 26), patients who underwent deceased donor liver transplantation (n = 9) and patients who underwent locoregional therapy more than 6 months prior to liver resection (n = 3). SLT, salvage liver transplantation; LR, liver resection; HCC, hepatocellular carcinoma; LT, liver transplantation; LRT, locoregional therapy.
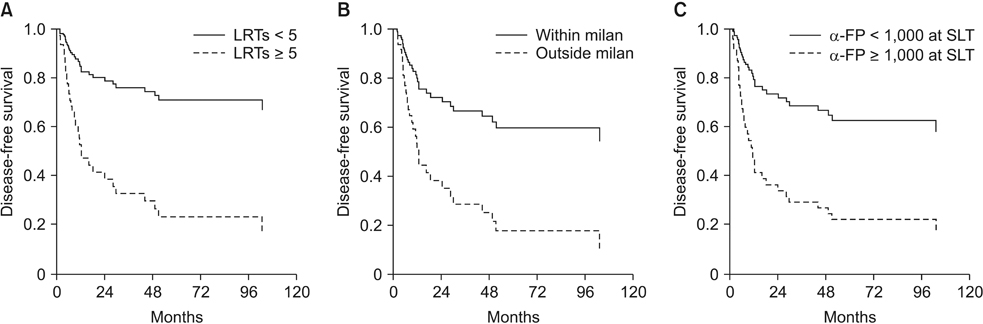
Fig. 2 Multivariate Cox analysis showed that patients who underwent 5 or more locoregional therapies prior to salvage liver transplantation (hazard ratio [HR], 3.74; 95% confidence interval [CI], 1.45–9.64, P = 0.006) (A) outside the Milan criteria at the time of transplantation (HR, 2.66, CI, 1.26–5.63, P = 0.011) (B) and α-FP level ≥ 1,000 ng/mL at the time of LT (HR, 3.43, CI, 1.28–9.18, P = 0.014) (C) were significant factors related to recurrence after salvage liver transplantation. HR, hazard ratio; CI, confidence interval; LRT, locoregional therapy; SLT, salvage liver transplantation.
Reference
-
1. Rustgi VK. Epidemiology of hepatocellular carcinoma. Gastroenterol Clin North Am. 1987; 16:545–551.
Article2. Ercolani G, Grazi GL, Ravaioli M, Del Gaudio M, Gardini A, Cescon M, et al. Liver resection for hepatocellular carcinoma on cirrhosis: univariate and multivariate analysis of risk factors for intrahepatic recurrence. Ann Surg. 2003; 237:536–543.3. Fong Y, Sun RL, Jarnagin W, Blumgart LH. An analysis of 412 cases of hepatocellular carcinoma at a Western center. Ann Surg. 1999; 229:790–799.
Article4. Poon RT, Fan ST, Lo CM, Ng IO, Liu CL, Lam CM, et al. Improving survival results after resection of hepatocellular carcinoma: a prospective study of 377 patients over 10 years. Ann Surg. 2001; 234:63–70.
Article5. Befeler AS, Di Bisceglie AM. Hepatocellular carcinoma: diagnosis and treatment. Gastroenterology. 2002; 122:1609–1619.
Article6. Bismuth H, Majno PE, Adam R. Liver transplantation for hepatocellular carcinoma. Semin Liver Dis. 1999; 19:311–322.
Article7. Yamamoto J, Iwatsuki S, Kosuge T, Dvorchik I, Shimada K, Marsh JW, et al. Should hepatomas be treated with hepatic resection or transplantation? Cancer. 1999; 86:1151–1158.
Article8. Majno PE, Sarasin FP, Mentha G, Hadengue A. Primary liver resection and salvage transplantation or primary liver transplantation in patients with single, small hepatocellular carcinoma and preserved liver function: an outcome-oriented decision analysis. Hepatology. 2000; 31:899–906.
Article9. Can MF, Hughes CB. Primary liver transplantation vs liver resection followed by transplantation for transplantable hepatocellular carcinoma: Liver functional quality and tumor characteristics matter. World J Gastrointest Surg. 2013; 5:5–8.10. Hu Z, Zhou J, Xu X, Li Z, Zhou L, Wu J, et al. Salvage liver transplantation is a reasonable option for selected patients who have recurrent hepatocellular carcinoma after liver resection. PLoS One. 2012; 7:e36587.
Article11. Lee S, Hyuck David Kwon C, Man Kim J, Joh JW, Woon Paik S, Kim BW, et al. Time of hepatocellular carcinoma recurrence after liver resection and alpha-fetoprotein are important prognostic factors for salvage liver transplantation. Liver Transpl. 2014; 20:1057–1063.
Article12. Shan Y, Huang L, Xia Q. Salvage liver transplantation leads to poorer outcome in hepatocellular carcinoma compared with primary liver transplantation. Sci Rep. 2017; 7:44652.
Article13. Wang P, Pu Y, Li H, Shi B, Zheng S, Zhong L. Prognosis for recipients with hepatocellular carcinoma of salvage liver transplantation versus those of primary liver transplantation: a retrospective single-center study. Springerplus. 2016; 5:1809.
Article14. Moon JI, Kwon CH, Joh JW, Choi GS, Jung GO, Kim JM, et al. Primary versus salvage living donor liver transplantation for patients with hepatocellular carcinoma: impact of microvascular invasion on survival. Transplant Proc. 2012; 44:487–493.
Article15. Yong CC, Tsai MC, Lin CC, Wang CC, Lu SN, Hung CH, et al. Comparison of salvage living donor liver transplantation and local regional therapy for recurrent hepatocellular carcinoma. World J Surg. 2016; 40:2472–2480.
Article16. Belghiti J, Cortes A, Abdalla EK, Régimbeau JM, Prakash K, Durand F, et al. Resection prior to liver transplantation for hepatocellular carcinoma. Ann Surg. 2003; 238:885–892.
Article17. Poon RT. Optimal initial treatment for early hepatocellular carcinoma in patients with preserved liver function: transplantation or resection. Ann Surg Oncol. 2007; 14:541–547.
Article18. Dai WC, Cheung TT. Strategic overview on the best treatment option for intrahepaitc hepatocellular carcinoma recurrence. Expert Rev Anticancer Ther. 2016; 16:1063–1072.
Article19. Yamashita Y, Yoshida Y, Kurihara T, Itoh S, Harimoto N, Ikegami T, et al. Surgical results for recurrent hepatocellular carcinoma after curative hepatectomy: repeat hepatectomy versus salvage living donor liver transplantation. Liver Transpl. 2015; 21:961–968.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Venous outflow congestion is related to poor recurrence-free survival of living donor liver transplantation recipients with hepatocellular carcinoma
- Liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis
- Management strategies for advanced hepatocellular carcinoma with portal vein tumor thrombosis
- Risk factors for poor survival after recurrence of hepatocellular carcinoma after liver transplantation
- Risk of posttransplantation recurrence in hepatocellular carcinoma patients within the Milan criteria: importance for evaluating the recurrence potential
