Clinical and Radiological Outcomes of Unilateral Biportal Endoscopic Decompression by 30° Arthroscopy in Lumbar Spinal Stenosis: Minimum 2-Year Follow-up
- Affiliations
-
- 1Department of Orthopedic Surgery, Andong Hospital, Andong, Korea. dspfuture@hanmail.net
- 2Department of Spine Surgery , Barun Hospital, Jinju, Korea.
- KMID: 2418753
- DOI: http://doi.org/10.4055/cios.2018.10.3.328
Abstract
- BACKGROUND
Open microscopic laminectomy has been the standard surgical method for degenerative spinal stenosis without instability till now. However, it is associated with complications such as paraspinal muscle injury, excessive bleeding, and wound infection. Several surgical techniques, including microendoscopic decompression, have been introduced to solve these problems.
METHODS
Authors analyzed retrospectively 55 patients presenting with neurological symptoms due to degenerative lumbar spinal stenosis refractory to conservative treatment. Patients with foraminal stenosis requiring foraminal decompression were excluded. Two or three portals were used for each level. One portal was used for viewing purpose and the others for instrument passage. Unilateral laminotomy was followed by bilateral decompression under the view of 30° arthroscopy. Clinical outcomes were evaluated using modified Macnab criteria, Oswestry disability index (ODI), and visual analogue scale (VAS). Postoperative complications were checked during the 2-year follow-up. Plain radiographs before and after surgery were compared to analyze the change of disc height decrement and alignment.
RESULTS
ODI scores improved from 67.4 ± 11.5 preoperatively to 19.3 ± 12.1 at 2-year follow-up (p < 0.01). VAS scores of the leg decreased from 7.7 ± 1.5 to 1.7 ± 1.5 at the final follow-up (p < 0.01). Per the modified Macnab criteria, 81% of the patients improved to good/excellent. No cases of infection occurred. The intervertebral angle was significantly reduced from 6.26°± 3.54° to 5.58°± 3.23° at 2 years postoperatively (p = 0.027) and the dynamic intervertebral angle changed from 6.54°± 3.71° to 6.76°± 3.59°, which was not statistically significant (p = 0.562). No significant change in slippage was observed (3.76% ± 5.01% preoperatively vs. 3.81% ± 5.28% at the final follow-up [p = 0.531]). The dynamic percentage slip did not change significantly, from 2.65% ± 3.37% to 2.76% ± 3.71% (p = 0.985). However, intervertebral distance decreased significantly from 10.43 ± 2.23 mm to 10.0 ± 2.24 mm (p = 0.000).
CONCLUSIONS
Full endoscopic decompression using a 30° arthroscopy demonstrated a satisfactory clinical outcome at the 2-year follow-up. This technique reduces wound infection rate and did not bring about postoperative segmental spinal instability. It could be a feasible alternative to conventional open microscopic decompression or fusion surgery for degenerative lumbar spinal stenosis.
Keyword
MeSH Terms
Figure
-
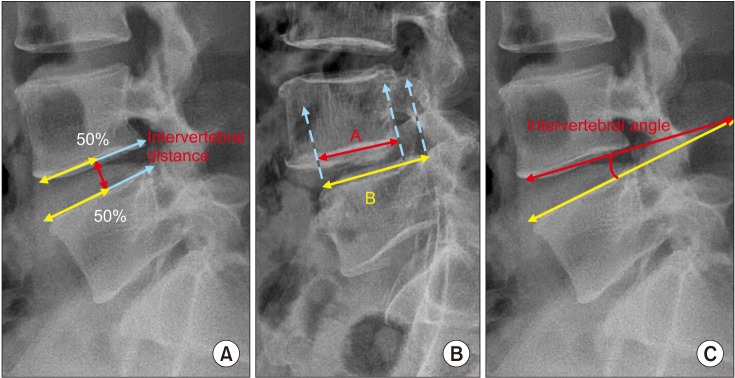
Fig. 1 Measurement of radiological data. (A) Intervertebral distance: vertical distance between the vertebrae at 50% (white line) of the anteroposterior diameter of each vertebral body (gray line). (B) Slip percentage: slip% = (B− A / B) × 100. White line: anteroposterior diameter of the vertebral body of the lower vertebra. Gray line: anteroposterior diameter of the vertebral body of the upper vertebra. Dotted line: end of vertebra. (C) Intervertebral angle.
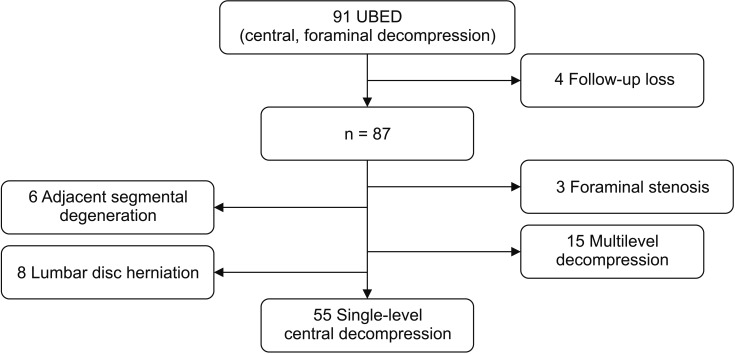
Fig. 2 Flowchart of patient inclusion. UBED: unilateral biportal endoscopic decompression.
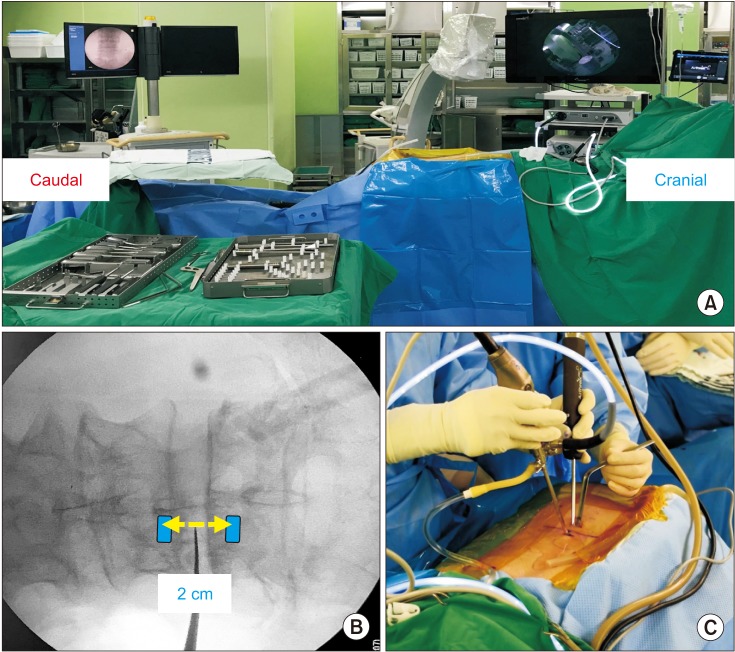
Fig. 3 (A) Setup for unilateral biportal endoscopic decompression surgery. (B) Locations of viewing (upper) and working (lower) portals. (C) Intraoperative photo showing the arthroscope and arthroscopic burr introduced through viewing and working portals.
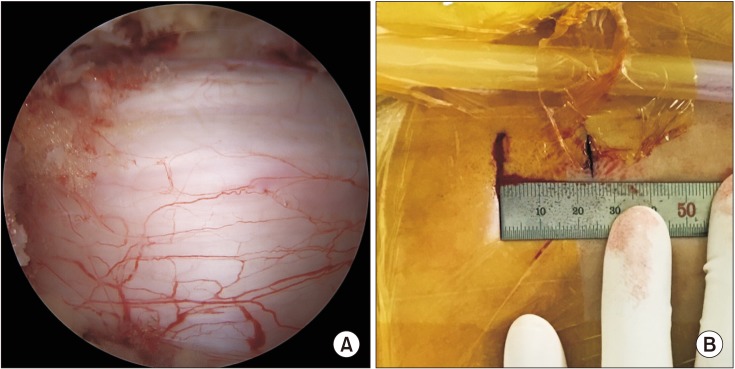
Fig. 4 (A) Intraoperative endoscopic image showing decompression of the central canal and ipsilateral laminotomy. (B) Postoperative photo showing the skin incision point in unilateral biportal endoscopic decompression.
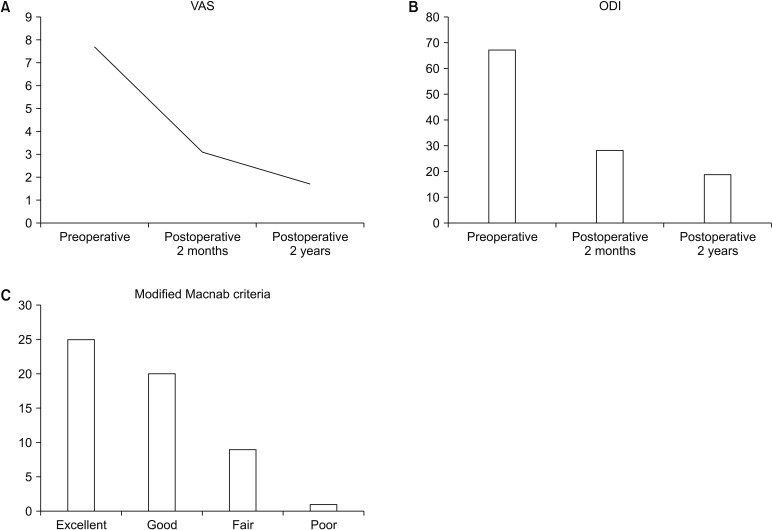
Fig. 5 (A) Visual analogue scale (VAS) pain scores assessed preoperatively and at 2 months and 2 years postoperatively. (B) Oswestry disability index (ODI) scores assessed preoperatively and at 2 months and 2 years postoperatively. (C) According to modified Macnab criteria, 81% of patients who underwent unilateral biportal endoscopic decompression experienced excellent or good results.
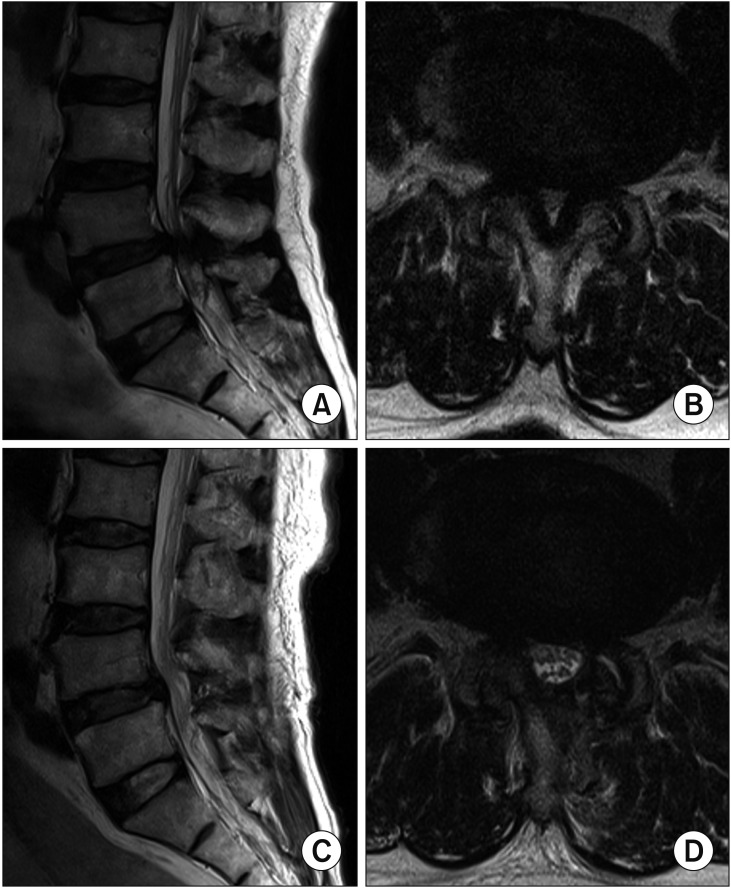
Fig. 6 Preoperative (A, B) and postoperative (C, D) T2-weighted magnetic resonance imaging scans obtained in a patient who underwent L4–5 decompression.
Cited by 1 articles
-
3D Printer Application for Endoscope-Assisted Spine Surgery Instrument Development: From Prototype Instruments to Patient-Specific 3D Models
Hee-Seok Yang, Jeong-Yoon Park
Yonsei Med J. 2020;61(1):94-99. doi: 10.3349/ymj.2020.61.1.94.
Reference
-
1. Weinstein JN, Tosteson TD, Lurie JD, et al. Surgical versus nonsurgical therapy for lumbar spinal stenosis. N Engl J Med. 2008; 358(8):794–810. PMID: 18287602.
Article2. Hu ZJ, Fang XQ, Zhou ZJ, Wang JY, Zhao FD, Fan SW. Effect and possible mechanism of muscle-splitting approach on multifidus muscle injury and atrophy after posterior lumbar spine surgery. J Bone Joint Surg Am. 2013; 95(24):e192(1-9). PMID: 24352778.
Article3. Huang YH, Ou CY. Significant blood loss in lumbar fusion surgery for degenerative spine. World Neurosurg. 2015; 84(3):780–785. PMID: 25986203.
Article4. Kim JY, Ryu DS, Paik HK, et al. Paraspinal muscle, facet joint, and disc problems: risk factors for adjacent segment degeneration after lumbar fusion. Spine J. 2016; 16(7):867–875. PMID: 26970600.
Article5. Iguchi T, Kurihara A, Nakayama J, Sato K, Kurosaka M, Yamasaki K. Minimum 10-year outcome of decompressive laminectomy for degenerative lumbar spinal stenosis. Spine (Phila Pa 1976). 2000; 25(14):1754–1759. PMID: 10888941.
Article6. Mariconda M, Fava R, Gatto A, Longo C, Milano C. Unilateral laminectomy for bilateral decompression of lumbar spinal stenosis: a prospective comparative study with conservatively treated patients. J Spinal Disord Tech. 2002; 15(1):39–46. PMID: 11891449.
Article7. Palmer S, Turner R, Palmer R. Bilateral decompression of lumbar spinal stenosis involving a unilateral approach with microscope and tubular retractor system. J Neurosurg. 2002; 97(2 Suppl):213–217. PMID: 12296681.
Article8. Cavusoglu H, Kaya RA, Turkmenoglu ON, Tuncer C, Colak I, Aydin Y. Midterm outcome after unilateral approach for bilateral decompression of lumbar spinal stenosis: 5-year prospective study. Eur Spine J. 2007; 16(12):2133–2142. PMID: 17712577.
Article9. Costa F, Sassi M, Cardia A, et al. Degenerative lumbar spinal stenosis: analysis of results in a series of 374 patients treated with unilateral laminotomy for bilateral microdecompression. J Neurosurg Spine. 2007; 7(6):579–586. PMID: 18074681.
Article10. Sasai K, Umeda M, Maruyama T, Wakabayashi E, Iida H. Microsurgical bilateral decompression via a unilateral approach for lumbar spinal canal stenosis including degenerative spondylolisthesis. J Neurosurg Spine. 2008; 9(6):554–559. PMID: 19035747.
Article11. Pao JL, Chen WC, Chen PQ. Clinical outcomes of microendoscopic decompressive laminotomy for degenerative lumbar spinal stenosis. Eur Spine J. 2009; 18(5):672–678. PMID: 19238459.
Article12. Choi CM, Chung JT, Lee SJ, Choi DJ. How I do it? Biportal endoscopic spinal surgery (BESS) for treatment of lumbar spinal stenosis. Acta Neurochir (Wien). 2016; 158(3):459–463. PMID: 26782827.
Article13. Hwa Eum J, Hwa Heo D, Son SK, Park CK. Percutaneous biportal endoscopic decompression for lumbar spinal stenosis: a technical note and preliminary clinical results. J Neurosurg Spine. 2016; 24(4):602–607. PMID: 26722954.
Article14. Baghdadi YM, Moussallem CD, Shuaib MA, Clarke MJ, Dekutoski MB, Nassr AN. Lumbar spinous process-splitting laminoplasty: a novel technique for minimally invasive lumbar decompression. Orthopedics. 2016; 39(5):e950–e956. PMID: 27337665.
Article15. Young S, Veerapen R, O'Laoire SA. Relief of lumbar canal stenosis using multilevel subarticular fenestrations as an alternative to wide laminectomy: preliminary report. Neurosurgery. 1988; 23(5):628–633. PMID: 3200393.
Article16. Turner JA, Ersek M, Herron L, Deyo R. Surgery for lumbar spinal stenosis: attempted meta-analysis of the literature. Spine (Phila Pa 1976). 1992; 17(1):1–8. PMID: 1531550.17. Kornblum MB, Fischgrund JS, Herkowitz HN, Abraham DA, Berkower DL, Ditkoff JS. Degenerative lumbar spondylolisthesis with spinal stenosis: a prospective long-term study comparing fusion and pseudarthrosis. Spine (Phila Pa 1976). 2004; 29(7):726–733. PMID: 15087793.18. Lipson SJ. Spinal-fusion surgery: advances and concerns. N Engl J Med. 2004; 350(7):643–644. PMID: 14960739.19. Jayarao M, Chin LS. Results after lumbar decompression with and without discectomy: comparison of the transspinous and conventional approaches. Neurosurgery. 2010; 66(3 Suppl Operative):152–160. PMID: 20173565.
Article20. Mobbs RJ, Li J, Sivabalan P, Raley D, Rao PJ. Outcomes after decompressive laminectomy for lumbar spinal stenosis: comparison between minimally invasive unilateral laminectomy for bilateral decompression and open laminectomy: clinical article. J Neurosurg Spine. 2014; 21(2):179–186. PMID: 24878273.21. Guiot BH, Khoo LT, Fessler RG. A minimally invasive technique for decompression of the lumbar spine. Spine (Phila Pa 1976). 2002; 27(4):432–438. PMID: 11840112.
Article22. Khoo LT, Fessler RG. Microendoscopic decompressive laminotomy for the treatment of lumbar stenosis. Neurosurgery. 2002; 51(5 Suppl):S146–S154. PMID: 12234442.
Article23. Lin PM. Internal decompression for multiple levels of lumbar spinal stenosis: a technical note. Neurosurgery. 1982; 11(4):546–549. PMID: 7145072.
Article24. Aryanpur J, Ducker T. Multilevel lumbar laminotomies: an alternative to laminectomy in the treatment of lumbar stenosis. Neurosurgery. 1990; 26(3):429–432. PMID: 2138716.
Article25. Weiner BK, Walker M, Brower RS, McCulloch JA. Microdecompression for lumbar spinal canal stenosis. Spine (Phila Pa 1976). 1999; 24(21):2268–2272. PMID: 10562995.
Article26. Spetzger U, Bertalanffy H, Reinges MH, Gilsbach JM. Unilateral laminotomy for bilateral decompression of lumbar spinal stenosis. Part II: clinical experiences. Acta Neurochir (Wien). 1997; 139(5):397–403. PMID: 9204107.
Article27. Thome C, Zevgaridis D, Leheta O, et al. Outcome after less-invasive decompression of lumbar spinal stenosis: a randomized comparison of unilateral laminotomy, bilateral laminotomy, and laminectomy. J Neurosurg Spine. 2005; 3(2):129–141. PMID: 16370302.28. Oertel MF, Ryang YM, Korinth MC, Gilsbach JM, Rohde V. Long-term results of microsurgical treatment of lumbar spinal stenosis by unilateral laminotomy for bilateral decompression. Neurosurgery. 2006; 59(6):1264–1269. PMID: 17277689.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Biportal Endoscopic Transforaminal Lumbar Interbody Fusion with Arthroscopy
- Clinical and Radiological Outcomes of Foraminal Decompression Using Unilateral Biportal Endoscopic Spine Surgery for Lumbar Foraminal Stenosis
- Biportal Percutaneous Endoscopic Spinal Surgery for Lumbar Spinal Stenosis
- Complications and Management of Endoscopic Spinal Surgery
- The Unilateral Biportal Endoscopic Technique for Treatment of Lumbar Spinal Stenosis: Early Surgical Results
