Clinical and Radiological Outcomes of Foraminal Decompression Using Unilateral Biportal Endoscopic Spine Surgery for Lumbar Foraminal Stenosis
- Affiliations
-
- 1Department of Orthopedic Surgery, Andong Hospital, Andong, Korea.
- 2Department of Orthopedic Surgery, Barun Hospital, Jinju, Korea.
- 3Department of Orthopedic Surgery, Chungnam National University Hospital, Chungnam National University School of Medicine, Daejeon, Korea. cnuhos55@hotmail.com
- KMID: 2426529
- DOI: http://doi.org/10.4055/cios.2018.10.4.439
Abstract
- BACKGROUND
Since open Wiltse approach allows limited visualization for foraminal stenosis leading to an incomplete decompression, we report the short-term clinical and radiological results of unilateral biportal endoscopic foraminal decompression using 0° or 30° endoscopy with better visualization.
METHODS
We examined 31 patients that underwent surgery for neurological symptoms due to lumbar foraminal stenosis which was refractory to 6 weeks of conservative treatment. All 31 patients underwent unilateral biportal endoscopic far-lateral decompression (UBEFLD). One portal was used for viewing purpose, and the other was for surgical instruments. Unilateral foraminotomy was performed under guidance of 0° or 30° endoscopy. Clinical outcomes were analyzed using the modified Macnab criteria, Oswestry disability index, and visual analogue scale. Plain radiographs obtained preoperatively and 1 year postoperatively were compared to analyze the intervertebral angle (IVA), dynamic IVA, percentage of slip, dynamic percentage of slip (gap between the percentage of slip on flexion and extension views), slip angle, disc height index (DHI), and foraminal height index (FHI).
RESULTS
The IVA significantly increased from 6.24°± 4.27° to 6.96°± 3.58° at 1 year postoperatively (p = 0.306). The dynamic IVA slightly decreased from 6.27°± 3.12° to 6.04°± 2.41°, but the difference was not statistically significant (p = 0.375). The percentage of slip was 3.41% ± 5.24% preoperatively and 6.01% ± 1.43% at 1-year follow-up (p = 0.227), showing no significant difference. The preoperative dynamic percentage of slip was 2.90% ± 3.37%; at 1 year postoperatively, it was 3.13% ± 4.11% (p = 0.720), showing no significant difference. The DHI changed from 34.78% ± 9.54% preoperatively to 35.05% ± 8.83% postoperatively, which was not statistically significant (p = 0.837). In addition, the FHI slightly decreased from 55.15% ± 9.45% preoperatively to 54.56% ± 9.86% postoperatively, but the results were not statistically significant (p = 0.705).
CONCLUSIONS
UBEFLD using endoscopy showed a satisfactory clinical outcome after 1-year follow-up and did not induce postoperative segmental spinal instability. It could be a feasible alternative to conventional open decompression or fusion surgery for lumbar foraminal stenosis.
Keyword
MeSH Terms
Figure
-
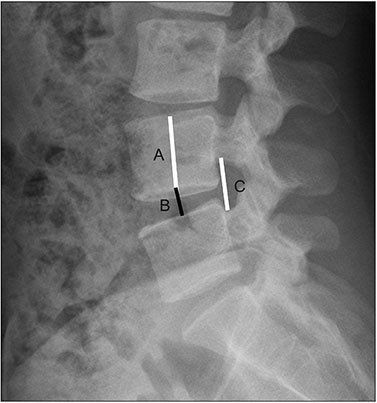
Fig. 1 Description of disc height index (B / A) and foraminal height index (C / A). A: vertebral body height measured at the midpoint of the body, B: disc height measured at the midpoint of the disc space, C: foraminal height measured as the largest distance between two adjacent pedicles.
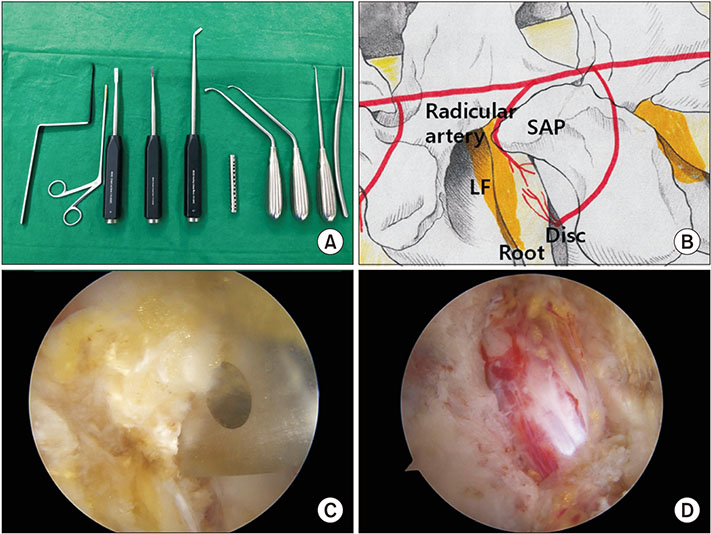
Fig. 2 (A) Surgical instruments used during surgery. Root retractor, pituitary forceps, three chisels with various angles, cannula for water outflow, curved and straight curettes, and a dilator (from left to right). (B) Schematic anatomy of the foraminal zone of the lumbar spine. Note the pathway of radicular artery and the shape of superior articular process. (C) Intraoperative image: superior articular process being removed using a chisel. (D) Intraoperative image: nerve root exposed after removal of the superior articular process. SAP: superior articular process, LF: ligamentum flavum.
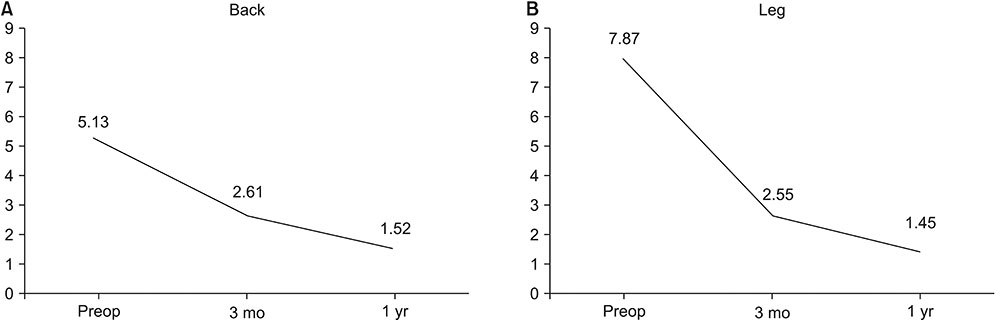
Fig. 3 Change of visual analogue scale score for back (A) and leg (B) from preoperative (Preop) to 3-month and 1-year postoperative assessments.
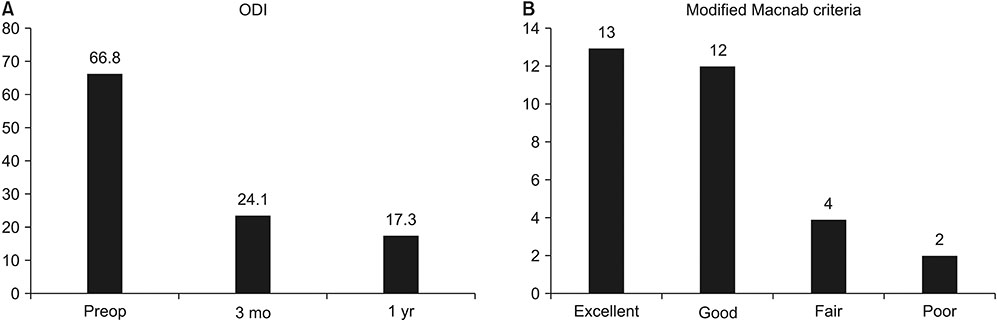
Fig. 4 (A) Change of Oswestry disability index (ODI) from preoperative (Preop) to 3-month and 1-year postoperative assessments. (B) Results according to modified Macnab criteria at 1 year postoperatively.

Fig. 5 Magnetic resonance images of one patient. (A) Preoperative parasagittal T1-weighted image of the left foramen. Note the compression of L5 nerve root. (B) Preoperative axial T2-weighted image. (C) Postoperative parasagittal T1-weighted image showing widened foraminal space for L5 nerve root. (D) Postoperative axial T2-weighted image. Note the removal of superior articular process and relatively widened left foraminal space.
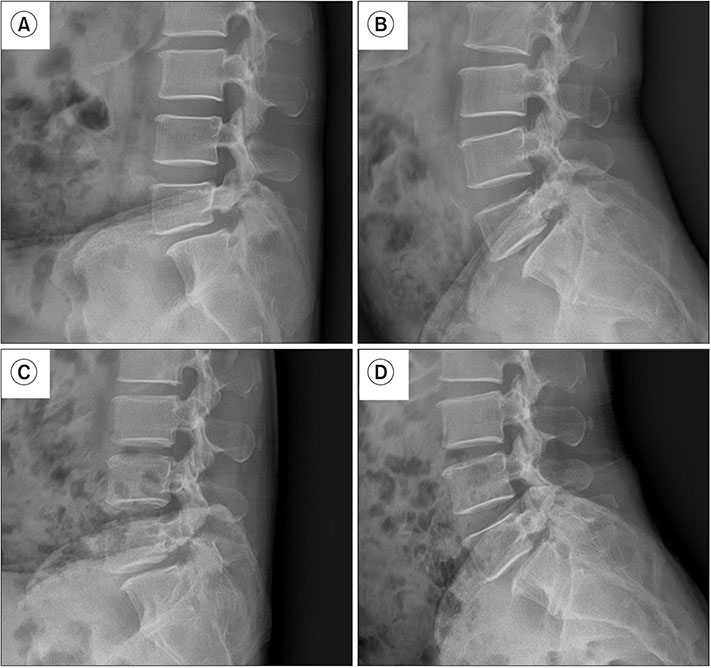
Fig. 6 A case with spondylolytic spondylolisthesis with foraminal stenosis. Preoperative flexion (A) and extension (B) images. Postoperative flexion (C) and extension (D) images.
Reference
-
1. Jenis LG, An HS. Spine update. Lumbar foraminal stenosis. Spine (Phila Pa 1976). 2000; 25(3):389–394.2. Ahn Y, Oh HK, Kim H, Lee SH, Lee HN. Percutaneous endoscopic lumbar foraminotomy: an advanced surgical technique and clinical outcomes. Neurosurgery. 2014; 75(2):124–133.3. Shenouda EF, Gill SS. Laminal fenestration for the treatment of lumbar nerve root foraminal stenosis. Br J Neurosurg. 2002; 16(5):494–496.
Article4. Chang SB, Lee SH, Ahn Y, Kim JM. Risk factor for unsatisfactory outcome after lumbar foraminal and far lateral microdecompression. Spine (Phila Pa 1976). 2006; 31(10):1163–1167.
Article5. Hallett A, Huntley JS, Gibson JN. Foraminal stenosis and single-level degenerative disc disease: a randomized controlled trial comparing decompression with decompression and instrumented fusion. Spine (Phila Pa 1976). 2007; 32(13):1375–1380.6. Kim HJ, Jeong JH, Cho HG, Chang BS, Lee CK, Yeom JS. Comparative observational study of surgical outcomes of lumbar foraminal stenosis using minimally invasive microsurgical extraforaminal decompression alone versus posterior lumbar interbody fusion: a prospective cohort study. Eur Spine J. 2015; 24(2):388–395.
Article7. Wiltse LL, Spencer CW. New uses and refinements of the paraspinal approach to the lumbar spine. Spine (Phila Pa 1976). 1988; 13(6):696–706.
Article8. Donaldson WF 3rd, Star MJ, Thorne RP. Surgical treatment for the far lateral herniated lumbar disc. Spine (Phila Pa 1976). 1993; 18(10):1263–1267.
Article9. Epstein NE. Foraminal and far lateral lumbar disc herniations: surgical alternatives and outcome measures. Spinal Cord. 2002; 40(10):491–500.
Article10. Kunogi J, Hasue M. Diagnosis and operative treatment of intraforaminal and extraforaminal nerve root compression. Spine (Phila Pa 1976). 1991; 16(11):1312–1320.
Article11. Hodges SD, Humphreys SC, Eck JC, Covington LA. The surgical treatment of far lateral L3-L4 and L4-L5 disc herniations: a modified technique and outcomes analysis of 25 patients. Spine (Phila Pa 1976). 1999; 24(12):1243–1246.12. Choi DJ, Jung JT, Lee SJ, Kim YS, Jang HJ, Yoo B. Biportal endoscopic spinal surgery for recurrent lumbar disc herniations. Clin Orthop Surg. 2016; 8(3):325–329.
Article13. Hwa Eum J, Hwa Heo D, Son SK, Park CK. Percutaneous biportal endoscopic decompression for lumbar spinal stenosis: a technical note and preliminary clinical results. J Neurosurg Spine. 2016; 24(4):602–607.
Article14. Soliman HM. Irrigation endoscopic decompressive laminotomy: a new endoscopic approach for spinal stenosis decompression. Spine J. 2015; 15(10):2282–2289.
Article15. Kim KT, Park SW, Kim YB. Disc height and segmental motion as risk factors for recurrent lumbar disc herniation. Spine (Phila Pa 1976). 2009; 34(24):2674–2678.
Article16. Baba H, Uchida K, Maezawa Y, Furusawa N, Okumura Y, Imura S. Microsurgical nerve root canal widening without fusion for lumbosacral intervertebral foraminal stenosis: technical notes and early results. Spinal Cord. 1996; 34(11):644–650.
Article17. Hu ZJ, Fang XQ, Zhou ZJ, Wang JY, Zhao FD, Fan SW. Effect and possible mechanism of muscle-splitting approach on multifidus muscle injury and atrophy after posterior lumbar spine surgery. J Bone Joint Surg Am. 2013; 95(24):e192(1-9).
Article18. Cavuşoğlu H, Turkmenoglu O, Kaya RA, et al. Efficacy of unilateral laminectomy for bilateral decompression in lumbar spinal stenosis. Turk Neurosurg. 2007; 17(2):100–108.19. Jayarao M, Chin LS. Results after lumbar decompression with and without discectomy: comparison of the transspinous and conventional approaches. Neurosurgery. 2010; 66:3 Suppl Operative. 152–160.
Article20. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine (Phila Pa 1976). 2008; 33(9):931–939.
Article21. Darden BV 2nd, Wade JF, Alexander R, Wood KE, Rhyne AL 3rd, Hicks JR. Far lateral disc herniations treated by microscopic fragment excision: techniques and results. Spine (Phila Pa 1976). 1995; 20(13):1500–1505.22. Gioia G, Mandelli D, Capaccioni B, Randelli F, Tessari L. Surgical treatment of far lateral lumbar disc herniation: identification of compressed root and discectomy by lateral approach. Spine (Phila Pa 1976). 1999; 24(18):1952–1957.23. Ahn Y, Lee SH, Park WM, Lee HY. Posterolateral percutaneous endoscopic lumbar foraminotomy for L5-S1 foraminal or lateral exit zone stenosis: technical note. J Neurosurg. 2003; 99:3 Suppl. 320–323.
Article24. Choi G, Lee SH, Bhanot A, Raiturker PP, Chae YS. Percutaneous endoscopic discectomy for extraforaminal lumbar disc herniations: extraforaminal targeted fragmentectomy technique using working channel endoscope. Spine (Phila Pa 1976). 2007; 32(2):E93–E99.25. Jang JS, An SH, Lee SH. Transforaminal percutaneous endoscopic discectomy in the treatment of foraminal and extraforaminal lumbar disc herniations. J Spinal Disord Tech. 2006; 19(5):338–343.
Article26. Knight M, Goswami A. Management of isthmic spondylolisthesis with posterolateral endoscopic foraminal decompression. Spine (Phila Pa 1976). 2003; 28(6):573–581.
Article27. Haufe SM, Mork AR. Effects of unilateral endoscopic facetectomy on spinal stability. J Spinal Disord Tech. 2007; 20(2):146–148.
Article28. Kiapour A, Ambati D, Hoy RW, Goel VK. Effect of graded facetectomy on biomechanics of Dynesys dynamic stabilization system. Spine (Phila Pa 1976). 2012; 37(10):E581–E589.
Article29. Youn MS, Shin JK, Goh TS, Lee JS. Clinical and radiological outcomes of endoscopic partial facetectomy for degenerative lumbar foraminal stenosis. Acta Neurochir (Wien). 2017; 159(6):1129–1135.
Article30. Ahn Y, Kim CH, Lee JH, Lee SH, Kim JS. Radiation exposure to the surgeon during percutaneous endoscopic lumbar discectomy: a prospective study. Spine (Phila Pa 1976). 2013; 38(7):617–625.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Current Status of Biportal Endoscopic Decompression for Lumbar Foraminal Stenosis: Endoscopic Partial Facetectomy and Outcome Factors
- Biportal Endoscopic Posterior Cervical Foraminotomy for Adjacent 2-Level Foraminal Lesions Using a Single Approach (Sliding Technique)
- Complications and Management of Endoscopic Spinal Surgery
- Management of a Rare Case of C2–3 Cervical Foraminal Disc Herniation by Unilateral Biportal Endoscopic Foraminotomy
- Treatment Concept and Technical Considerations of Biportal Endoscopic Spine Surgery for Lumbar Spinal Stenosis
