Yeungnam Univ J Med.
2018 Jun;35(1):70-75. 10.12701/yujm.2018.35.1.70.
Risk factors for persistent otitis media with effusion in children: a case-control study
- Affiliations
-
- 1Department of Pediatrics, Jeju National University Hospital, Jeju, Korea.
- 2Department of Otorhinolaryngology, Jeju National University School of Medicine, Jeju, Korea.
- 3Department of Laboratory Medicine, Jeju National University School of Medicine, Jeju, Korea.
- 4Department of Pediatrics, Jeju National University School of Medicine, Jeju, Korea. jhchoi@jejunu.ac.kr
- KMID: 2415736
- DOI: http://doi.org/10.12701/yujm.2018.35.1.70
Abstract
- BACKGROUND
Otitis media with effusion (OME) is defined as middle ear effusion without acute signs of infection. OME usually resolves spontaneously; however, persistent OME may require the insertion of a ventilation tube. This study investigated risk factors for persistent OME in children who undergo ventilation tube insertion.
METHODS
Children who were admitted to undergo ventilation tube insertion at Jeju National University Hospital between August 2015 and July 2016 were enrolled as the case group. Healthy children without persistent OME from August 2016 to July 2017 were enrolled as the control group. Baseline characteristics and predisposing factor data were collected using an interview questionnaire. Middle ear fluids were collected from the case group.
RESULTS
A total of 31 patients underwent ventilation tube insertion. The mean age of the case group was 4.53 years, with a male-to-female ratio of 21:10. Twenty-nine (93.5%) children attended a daycare center, and 21 (67.7%) had experience with bottle feeding. Fifteen (48.4%) children in the case group and 3 (9.7%) in the control group first attended a daycare center at < 1 year of age (odds ratio=9.96; 95% confidence interval=2.44-39.70; p=0.001). No bacteria were found in middle ear fluid collected from the 31 operated children. Nasopharyngeal bacterial colonization was found in 13 (41.9%) and 17 (54.8%) children in the case and control groups, respectively.
CONCLUSION
Earlier attendance at a daycare center was the only predisposing factor for ventilation tube insertion in our study. The aseptic nature of middle ear fluids found in children with OME highlights the efficacy of antimicrobial use.
MeSH Terms
Figure
-
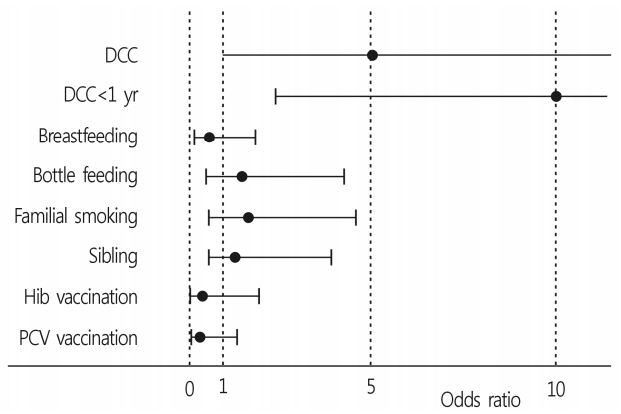
Fig. 1. Odds ratio of patient characteristics who underwent ventilation tube insertion. DCC, daycare center; Hib, Haemophilus influenzae type b; PCV, pneumococcal conjugate vaccine.
Reference
-
1. Teele DW, Klein JO, Rosner BA. Epidemiology of otitis media in children. Ann Otol Rhinol Laryngol Suppl. 1980; 89:5–6.
Article2. Williamson IG, Dunleavey J, Bain J, Robinson D. The natural history of otitis media with effusion--a three-year study of the incidence and prevalence of abnormal tympanograms in four South West Hampshire infant and first schools. J Laryngol Otol. 1994; 108:930–4.3. Tos M. Epidemiology and natural history of secretory otitis. Am J Otol. 1984; 5:459–62.4. Rosenfeld RM, Shin JJ, Schwartz SR, Coggins R, Gagnon L, Hackell JM, et al. Clinical practice guideline: otitis media with effusion (update). Otolaryngol Head Neck Surg. 2016; 154(1 Suppl):S1–41.
Article5. Rosenfeld RM, Schwartz SR, Pynnonen MA, Tunkel DE, Hussey HM, Fichera JS, et al. Clinical practice guideline: Tympanostomy tubes in children. Otolaryngol Head Neck Surg. 2013; 149(1 Suppl):S1–35.6. Williamson I. Otitis media with effusion in children. BMJ Clin Evid. 2011; 2011:pii: 0502.7. Owen MJ, Baldwin CD, Swank PR, Pannu AK, Johnson DL, Howie VM. Relation of infant feeding practices, cigarette smoke exposure, and group child care to the onset and duration of otitis media with effusion in the first two years of life. J Pediatr. 1993; 123:702–11.
Article8. Alles R, Parikh A, Hawk L, Darby Y, Romero JN, Scadding G. The prevalence of atopic disorders in children with chronic otitis media with effusion. Pediatr Allergy Immunol. 2001; 12:102–6.
Article9. Gok U, Bulut Y, Keles E, Yalcin S, Doymaz MZ. Bacteriological and PCR analysis of clinical material aspirated from otitis media with effusions. Int J Pediatr Otorhinolaryngol. 2001; 60:49–54.
Article10. Kreiner-Møller E, Chawes BL, Caye-Thomasen P, Bønnelykke K, Bisgaard H. Allergic rhinitis is associated with otitis media with effusion: a birth cohort study. Clin Exp Allergy. 2012; 42:1615–20.
Article11. Faden H, Duffy L, Wasielewski R, Wolf J, Krystofik D, Tung Y. Relationship between nasopharyngeal colonization and the development of otitis media in children. J Infect Dis. 1997; 175:1440–5.
Article12. García-Rodríguez JA, Fresnadillo Martínez MJ. Dynamics of nasopharyngeal colonization by potential respiratory pathogens. J Antimicrob Chemother. 2002; 50(Suppl S2):59–73.
Article13. Korean Otologic Society. Korean clinical practive guideline: otitis media in children 2014 [Internet]. Seoul: Korean Medical Guideline Information Center;2014. [cited 2018 April 3]. http://www.otologicalsociety.or.kr.14. Ahn JH, Yoon TH, Pae KH, Kim TS, Chung JW, Lee KS. Clinical manifestations and risk factors of children receiving triple ventilating tube insertions for treatment of recurrent otitis media with effusion. Pediatrics. 2006; 117:e1119. –23.
Article15. Pestalozza G, Romagnoli M, Tessitore E. Incidence and risk factors of acute otitis media and otitis media with effusion in children of different age groups. Adv Otorhinolaryngol. 1988; 40:47–56.
Article16. Casselbrant ML, Mandel EM, Doyle WJ. Information on comorbidities collected by history is useful for assigning Otitis Media risk to children. Int J Pediatr Otorhinolaryngol. 2016; 85:136–40.
Article17. Kim EJ, Kwon YR, Song KH, Jang WN, Lee J, Chang JK, et al. A study on risk factors of recurrent otitis media. Korean J Pediatr Infect Dis. 2010; 17:91–100. Korean.
Article18. Rovers MM, Zielhuis GA, Ingels K, van der Wilt GJ. Day-care and otitis media in young children: a critical overview. Eur J Pediatr. 1999; 158:1–6.19. Khanna R, Lakhanpaul M, Bull PD; Guideline Development Group. Surgical management of otitis media with effusion in children: summary of NICE guidance. Clin Otolaryngol. 2008; 33:600–5.
Article20. Poetker DM, Lindstrom DR, Edmiston CE, Krepel CJ, Link TR, Kerschner JE. Microbiology of middle ear effusions from 292 patients undergoing tympanostomy tube placement for middle ear disease. Int J Pediatr Otorhinolaryngol. 2005; 69:799–804.
Article21. Kim SH, Jeon EJ, Hong SM, Bae CH, Lee HY, Park MK, et al. Bacterial species and antibiotic sensitivity in korean patients diagnosed with acute otitis media and otitis media with effusion. J Korean Med Sci. 2017; 32:672–8.
Article22. Holder RC, Kirse DJ, Evans AK, Peters TR, Poehling KA, Swords WE, et al. One third of middle ear effusions from children undergoing tympanostomy tube placement had multiple bacterial pathogens. BMC Pediatr. 2012; 12:87.
Article23. Ngo CC, Massa HM, Thornton RB, Cripps AW. Predominant bacteria detected from the middle ear fluid of children experiencing otitis media: a systematic review. PLoS One. 2016; 11:e0150949.
Article24. Farajzadah Sheikh A, Saki N, Roointan M, Ranjbar R, Yadyad MJ, Kaydani A, et al. Identification of Alloiococcus otitidis, Streptococcus pneumoniae, Moraxella catarrhalis and Haemophilus influenzae in children with otitis media with effusion. Jundishapur J Microbiol. 2015; 8:e17985.
Article25. Jervis-Bardy J, Carney AS, Duguid R, Leach AJ. Microbiology of otitis media in Indigenous Australian children: review. J Laryngol Otol. 2017; 131(S2):S2–11.
Article26. Mills N, Best EJ, Murdoch D, Souter M, Neeff M, Anderson T, et al. What is behind the ear drum? The microbiology of otitis media and the nasopharyngeal flora in children in the era of pneumococcal vaccination. J Paediatr Child Health. 2015; 51:300–6.
Article27. Nourizadeh N, Ghazvini K, Gharavi V, Nourizadeh N, Movahed R. Evaluation of nasopharyngeal microbial flora and antibiogram and its relation to otitis media with effusion. Eur Arch Otorhinolaryngol. 2016; 273:859–63.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Middle ear histopathology in children with otitis media with effusion
- Decreased Serum Immunoglobulin in Recurrent Otitis Media with Effusion
- Adult-onset Otitis Media with Effusion
- Development of Animal Models of Otitis Media
- A Prevalence Study of Otitis Media with Effusion in Kindergarten Children in Puchun
