Successful rapid drug desensitization to methotrexate in a patient with primary central nervous system lymphoma
- Affiliations
-
- 1Department of Internal Medicine, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- 2Department of Oncology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea. csuh@amc.seoul.kr
- 3Department of Allergy and Clinical Immunology, Asan Medical Center, University of Ulsan College of Medicine, Seoul, Korea.
- KMID: 2414367
- DOI: http://doi.org/10.5045/br.2018.53.1.71
Abstract
- No abstract available.
Figure
-

Fig. 1 Hypersensitivity skin reaction after methotrexate infusion. After 30 minutes of methotrexate infusion, urticarial rashes developed in the face, neck, and anterior chest area.
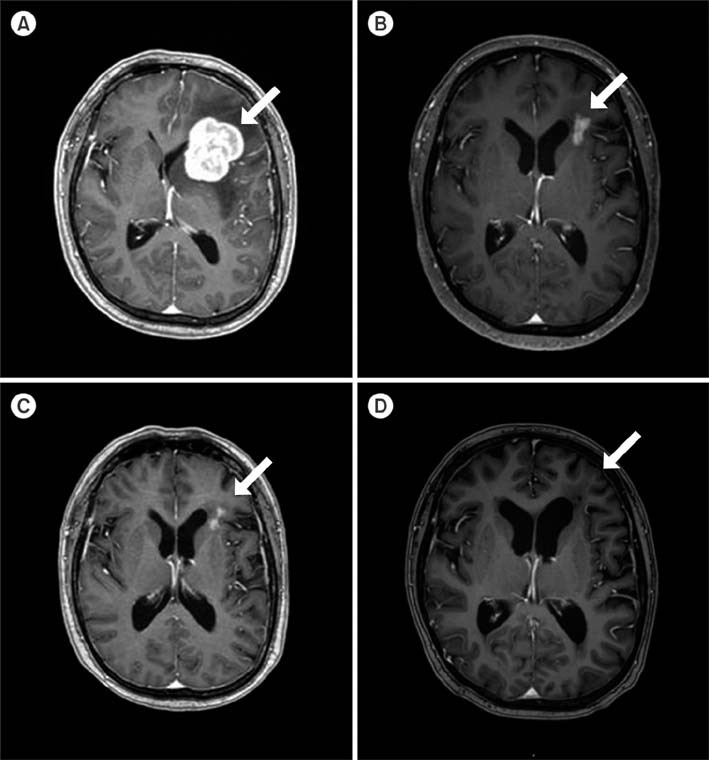
Fig. 2 MRI changes in the lymphoma lesion during chemotherapy. Prior to receiving chemotherapy, the size of the frontal lesion was approximately 4.1 cm with perilesional edema and midline shifting to the right side (A). After the fourth cycle of chemotherapy, partial remission was achieved, with decrease in tumor size to approximately 2.1 cm with perilesional edema as well as disappearance of midline shifting (B). After the sixth cycle of chemotherapy, the tumor further decreased to 1.8 cm with perilesional edema (C). After undergoing ASCT, the patient achieved CR (D).
Reference
-
1. Pugi A, Benemei S, Vietri M, et al. Anaphylaxis during the first course of high-dose methotrexate: a case report and literature review. J Clin Pharm Ther. 2012; 37:245–248.
Article2. Ferreri AJ. How I treat primary CNS lymphoma. Blood. 2011; 118:510–522.
Article3. Ring J, Behrendt H. Anaphylaxis and anaphylactoid reactions. Classification and pathophysiology. Clin Rev Allergy Immunol. 1999; 17:387–399.4. Ring J, Behrendt H, de Weck A. History and classification of anaphylaxis. Chem Immunol Allergy. 2010; 95:1–11.
Article5. Hoang-Xuan K, Bessell E, Bromberg J, et al. Diagnosis and treatment of primary CNS lymphoma in immunocompetent patients: guidelines from the European Association for Neuro-Oncology. Lancet Oncol. 2015; 16:e322–e332.
Article6. Oulego-Erroz I, Maneiro-Freire M, Bouzón-Alejandro M, Vázquez-Donsión M, Couselo JM. Anaphylactoid reaction to high-dose methotrexate and successful desensitization. Pediatr Blood Cancer. 2010; 55:557–559.
Article7. Davis KA, Williams P, Walker JC. Successful desensitization to high-dose methotrexate after systemic anaphylaxis. Ann Allergy Asthma Immunol. 2003; 90:87–89.
Article8. MacGinnitie AJ, Walensky LD, Turvey SE, et al. Management of an anaphylactoid reaction to methotrexate with a stepwise graded challenge. Pediatr Allergy Immunol. 2003; 14:409–411.
Article9. Bouchireb K, Dodille A, Ponvert C, Gouraud F, Dubrel M, Brugières L. Management and successful desensitization in methotrexate-induced anaphylaxis. Pediatr Blood Cancer. 2009; 52:295–297.
Article10. del Carmen Sancho M, Breslow R, Sloane D, Castells M. Desensitization for hypersensitivity reactions to medications. Chem Immunol Allergy. 2012; 97:217–233.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Experience of Childhood Non-Hodgkin Lymphoma with Central Nervous System Involvement at Diagnosis
- A Case of the Cauda Equina Syndrome Associated With the Intrathecal Chemotherapy in a Patient With Primary Central Nervous System Lymphoma
- Primary Central Nervous System Lymphoma in Organ Recipient
- A Case of Primary Central Nervous System Lymphoma Located at Brain Stem in a Child
- Recent advances in the management of primary central nervous system lymphoma
