Endocrinol Metab.
2017 Mar;32(1):83-89. 10.3803/EnM.2017.32.1.83.
Clinical Characteristics of Patients with Adrenal Insufficiency in a General Hospital
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Keimyung University School of Medicine, Daegu, Korea. mdkmk@dsmc.or.kr
- KMID: 2413291
- DOI: http://doi.org/10.3803/EnM.2017.32.1.83
Abstract
- BACKGROUND
Adrenal insufficiency (AI) is a life-threatening disorder caused by the deficiency of adrenal steroid hormones. This retrospective cross-sectional study investigated the characteristics of patients with AI in Korea.
METHODS
All consecutive patients with suspected AI who received care at a tertiary referral center in Korea in 2014 and underwent adrenocorticotropic hormone stimulation or insulin-tolerance testing were identified through a review of medical charts. Patients diagnosed with AI were enrolled. Their demographic, clinical, and treatment details were extracted.
RESULTS
Of 771 patients with suspected AI, 183 (23.7%) received a definitive diagnosis. The most common reason for testing was the presence of suspicious AI-related symptoms (30.0%), followed by a history of steroid medications (23.5%). Their mean age was 66.7 years, and females predominated (67.8%). The most common symptoms were general weakness, anorexia, arthralgia, and fever. Approximately half (53.6%) had a history of steroid use. Hydrocortisone was the most common treatment (71.6%), with most patients taking a 30 mg dose (44.2%). The most common dose frequency was twice a day (78.6%). Fourteen patients were treated for adrenal crisis (n=10, 5.5%) or an intercurrent illness (n=4, 2.2%).
CONCLUSION
AI may have been caused by steroid medication use in many of the patients included in this study. The detection of AI can be improved by careful history-taking and being alert to the possibility that a patient has used steroids.
MeSH Terms
Figure
-
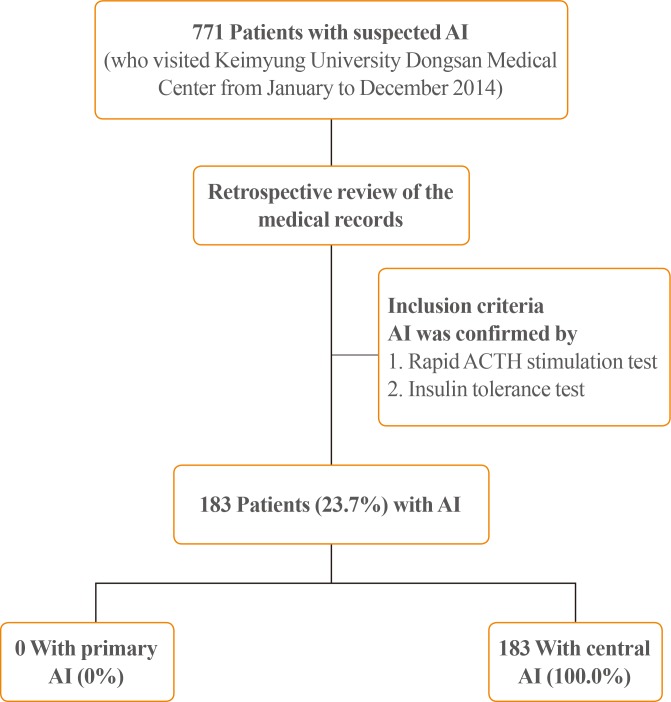
Fig. 1 Flow chart showing the disposition of patients with adrenal insufficiency (AI) in the study. ACTH, adrenocorticotropic hormone.
Cited by 1 articles
-
Encountering COVID-19 as Endocrinologists
Eun-Jung Rhee, Jung Hee Kim, Sun Joon Moon, Won-Young Lee
Endocrinol Metab. 2020;35(2):197-205. doi: 10.3803/EnM.2020.35.2.197.
Reference
-
2. Bornstein SR. Predisposing factors for adrenal insufficiency. N Engl J Med. 2009; 360:2328–2339. PMID: 19474430.
Article3. Neary N, Nieman L. Adrenal insufficiency: etiology, diagnosis and treatment. Curr Opin Endocrinol Diabetes Obes. 2010; 17:217–223. PMID: 20375886.
Article4. Charmandari E, Nicolaides NC, Chrousos GP. Adrenal insufficiency. Lancet. 2014; 383:2152–2167. PMID: 24503135.
Article5. Addison T. On the constitutional and local effects of disease of the supra-renal capsules. London: Samuel Highley;1855.6. Sarett LH. Partial synthesis of pregnene-4-triol-17(beta), 20(beta), 21-dione-3,11 and pregnene-4-diol-17(beta), 21-trione-3,11,20 monoacetate. J Biol Chem. 1946; 162:601–631. PMID: 21018769.7. Kendall EC. Hormones of the adrenal cortex in health and disease. Proc Am Philos Soc. 1953; 97:8–11.8. Hillier SG. Diamonds are forever: the cortisone legacy. J Endocrinol. 2007; 195:1–6. PMID: 17911391.
Article9. Dorin RI, Qualls CR, Crapo LM. Diagnosis of adrenal insufficiency. Ann Intern Med. 2003; 139:194–204. PMID: 12899587.
Article10. Burke CW. Adrenocortical insufficiency. Clin Endocrinol Metab. 1985; 14:947–976. PMID: 3002680.
Article12. Grossman AB. Clinical review. The diagnosis and management of central hypoadrenalism. J Clin Endocrinol Metab. 2010; 95:4855–4863. PMID: 20719838.13. Ekman B, Fitts D, Marelli C, Murray RD, Quinkler M, Zelissen PM. European Adrenal Insufficiency Registry (EU-AIR): a comparative observational study of glucocorticoid replacement therapy. BMC Endocr Disord. 2014; 14:40. PMID: 24884782.
Article14. Kong MF, Jeffcoate W. Eighty-six cases of Addison's disease. Clin Endocrinol (Oxf). 1994; 41:757–761. PMID: 7889611.
Article15. Willis AC, Vince FP. The prevalence of Addison's disease in Coventry, UK. Postgrad Med J. 1997; 73:286–288. PMID: 9196701.
Article16. Laureti S, Vecchi L, Santeusanio F, Falorni A. Is the prevalence of Addison's disease underestimated? J Clin Endocrinol Metab. 1999; 84:1762. PMID: 10323417.
Article17. Nilsson B, Gustavasson-Kadaka E, Bengtsson BA, Jonsson B. Pituitary adenomas in Sweden between 1958 and 1991: incidence, survival, and mortality. J Clin Endocrinol Metab. 2000; 85:1420–1425. PMID: 10770176.
Article18. Regal M, Paramo C, Sierra SM, Garcia-Mayor RV. Prevalence and incidence of hypopituitarism in an adult Caucasian population in northwestern Spain. Clin Endocrinol (Oxf). 2001; 55:735–740. PMID: 11895214.
Article19. Bates AS, Van't Hoff W, Jones PJ, Clayton RN. The effect of hypopituitarism on life expectancy. J Clin Endocrinol Metab. 1996; 81:1169–1172. PMID: 8772595.
Article20. Tomlinson JW, Holden N, Hills RK, Wheatley K, Clayton RN, Bates AS, et al. Association between premature mortality and hypopituitarism. West Midlands Prospective Hypopituitary Study Group. Lancet. 2001; 357:425–431. PMID: 11273062.21. Coursin DB, Wood KE. Corticosteroid supplementation for adrenal insufficiency. JAMA. 2002; 287:236–240. PMID: 11779267.
Article22. Yoo SJ, Jeong H. Diagnosis and treatment of adrenal insufficiency. Hanyang Med Rev. 2012; 32:203–212.
Article23. Rosen T, Bengtsson BA. Premature mortality due to cardiovascular disease in hypopituitarism. Lancet. 1990; 336:285–288. PMID: 1973979.24. Rosmond R, Bjorntorp P. The hypothalamic-pituitary-adrenal axis activity as a predictor of cardiovascular disease, type 2 diabetes and stroke. J Intern Med. 2000; 247:188–197. PMID: 10692081.
Article25. Korea Centers for Disease Control and Prevention. Korea Health Statistics 2015: Korea National Health and Nutrition Examination Survey (KNHANES VI-3). . Cheongju: Korea Centers for Disease Control and Prevention;2015.28. Krasner AS. Glucocorticoid-induced adrenal insufficiency. JAMA. 1999; 282:671–676. PMID: 10517721.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinical Characteristics of Patients with Adrenal Insufficiency and Fever
- Hemodynamic Instability due to Adrenal Insufficiency after Open Heart Surgery
- Adrenal Tuberculosis Mimicking a Malignant Tumor with Primary Adrenal Insufficiency
- Secondary Adrenal Insufficiency Associated with Megestrol Acetate in a Patient with Lung Cancer
- A Case of Adrenal Aplasia
