Endocrinol Metab.
2017 Mar;32(1):68-76. 10.3803/EnM.2017.32.1.68.
Site-Specific Difference of Bone Geometry Indices in Hypoparathyroid Patients
- Affiliations
-
- 1Division of Endocrinology and Metabolism, Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. lsk@yuhs.ac
- KMID: 2413289
- DOI: http://doi.org/10.3803/EnM.2017.32.1.68
Abstract
- BACKGROUND
Hypoparathyroid patients often have a higher bone mineral density (BMD) than the general population. However, an increase in BMD does not necessarily correlate with a solid bone microstructure. This study aimed to evaluate the bone microstructure of hypoparathyroid patients by using hip structure analysis (HSA).
METHODS
Ninety-five hypoparathyroid patients >20 years old were enrolled and 31 of them had eligible data for analyzing bone geometry parameters using HSA. And among the control data, we extracted sex-, age-, and body mass index-matched three control subjects to each patient. The BMD data were reviewed retrospectively and the bone geometry parameters of the patients were analyzed by HSA.
RESULTS
The mean Z-scores of hypoparathyroid patients at the lumbar spine, femoral neck, and total hip were above zero (0.63±1.17, 0.48±1.13, and 0.62±1.10, respectively). The differences in bone geometric parameters were site specific. At the femoral neck and intertrochanter, the cross-sectional area (CSA) and cortical thickness (C.th) were higher, whereas the buckling ratio (BR) was lower than in controls. However, those trends were opposite at the femoral shaft; that is, the CSA and C.th were low and the BR was high.
CONCLUSION
Our study shows the site-specific effects of hypoparathyroidism on the bone. Differences in bone components, marrow composition, or modeling based bone formation may explain these findings. However, further studies are warranted to investigate the mechanism, and its relation to fracture risk.
MeSH Terms
Figure
-
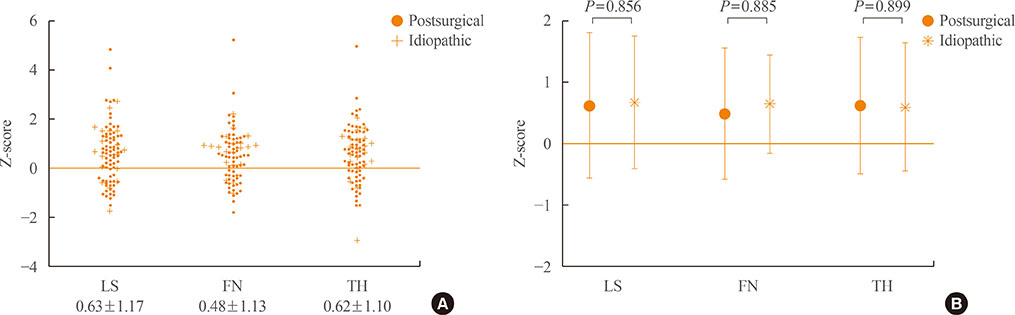
Fig. 1 Z-scores of the hypoparathyroid patients. (A) Distribution of the Z-scores of hypoparathyroid patients. (B) Z-scores according to disease etiology. Symbols represent mean±SD. LS, lumbar spine; FN, femoral neck; TH, total hip.
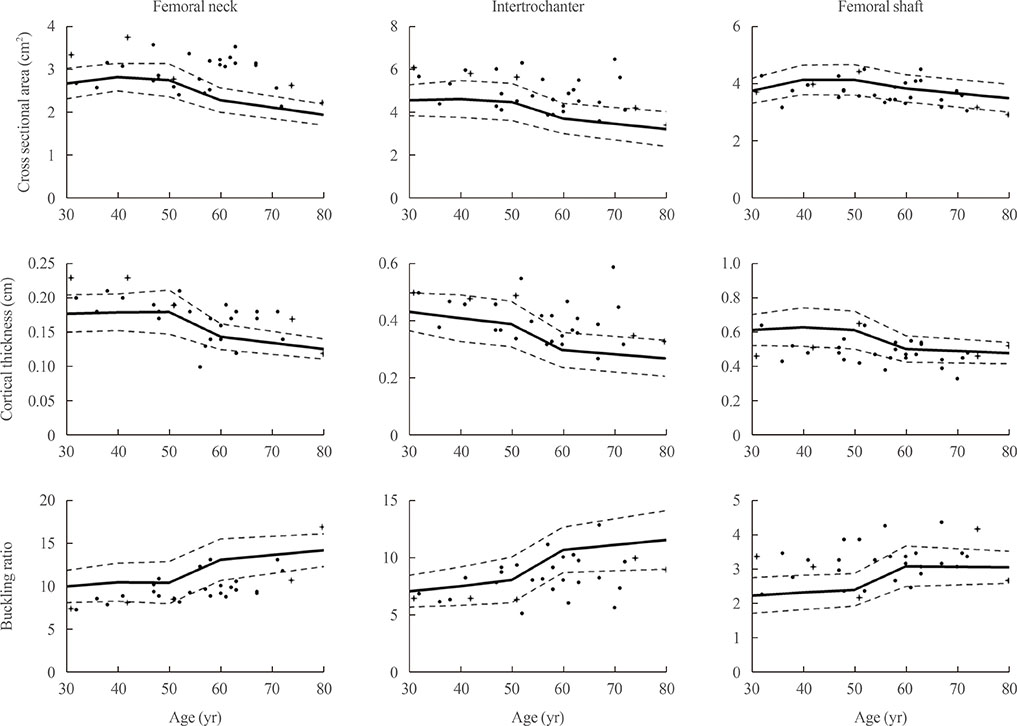
Fig. 2 Bone geometric parameters of the control subjects and hypoparathyroid patients. The values of the sex-, age-, and body mass index-matched control subjects are depicted as lines shown as mean±SD; those of the hypoparathyroid patients are shown as circles (postsurgical hypoparathyroidism) or cross (idiopathic hypoparathyroidism).
Reference
-
1. Cusano NE, Rubin MR, Bilezikian JP. Parathyroid hormone therapy for hypoparathyroidism. Best Pract Res Clin Endocrinol Metab. 2015; 29:47–55.2. Ma YL, Cain RL, Halladay DL, Yang X, Zeng Q, Miles RR, et al. Catabolic effects of continuous human PTH (1-38) in vivo is associated with sustained stimulation of RANKL and inhibition of osteoprotegerin and gene-associated bone formation. Endocrinology. 2001; 142:4047–4054.3. Fu Q, Jilka RL, Manolagas SC, O'Brien CA. Parathyroid hormone stimulates receptor activator of NFkappa B ligand and inhibits osteoprotegerin expression via protein kinase A activation of cAMP-response element-binding protein. J Biol Chem. 2002; 277:48868–48875.4. Aslan D, Andersen MD, Gede LB, de Franca TK, Jorgensen SR, Schwarz P, et al. Mechanisms for the bone anabolic effect of parathyroid hormone treatment in humans. Scand J Clin Lab Invest. 2012; 72:14–22.5. Lewiecki EM, Miller PD. Skeletal effects of primary hyperparathyroidism: bone mineral density and fracture risk. J Clin Densitom. 2013; 16:28–32.6. Chan FK, Tiu SC, Choi KL, Choi CH, Kong AP, Shek CC. Increased bone mineral density in patients with chronic hypoparathyroidism. J Clin Endocrinol Metab. 2003; 88:3155–3159.7. Takamura Y, Miyauchi A, Yabuta T, Kihara M, Ito Y, Miya A. Attenuation of postmenopausal bone loss in patients with transient hypoparathyroidism after total thyroidectomy. World J Surg. 2013; 37:2860–2865.8. Underbjerg L, Sikjaer T, Mosekilde L, Rejnmark L. Postsurgical hypoparathyroidism: risk of fractures, psychiatric diseases, cancer, cataract, and infections. J Bone Miner Res. 2014; 29:2504–2510.9. Mendonca ML, Pereira FA, Nogueira-Barbosa MH, Monsignore LM, Teixeira SR, Watanabe PC, et al. Increased vertebral morphometric fracture in patients with postsurgical hypoparathyroidism despite normal bone mineral density. BMC Endocr Disord. 2013; 13:1.10. Underbjerg L, Sikjaer T, Mosekilde L, Rejnmark L. The epidemiology of nonsurgical hypoparathyroidism in Denmark: a nationwide case finding study. J Bone Miner Res. 2015; 30:1738–1744.11. Cusano NE, Nishiyama KK, Zhang C, Rubin MR, Boutroy S, McMahon DJ, et al. Noninvasive assessment of skeletal microstructure and estimated bone strength in hypoparathyroidism. J Bone Miner Res. 2016; 31:308–316.12. Kim KM, Lim JS, Kim KJ, Choi HS, Rhee Y, Oh HJ, et al. Dissimilarity of femur aging in men and women from a Nationwide Survey in Korea (KNHANES IV). J Bone Miner Metab. 2013; 31:144–152.13. Kim KM, Kim YJ, Choi SH, Lim S, Moon JH, Kim JH, et al. The effects of body mass index on the hereditary influences that determine peak bone mass in mother-daughter pairs (KNHANES V). Osteoporos Int. 2016; 27:2057–2064.14. Uusi-Rasi K, Semanick LM, Zanchetta JR, Bogado CE, Eriksen EF, Sato M, et al. Effects of teriparatide [rhPTH (1-34)] treatment on structural geometry of the proximal femur in elderly osteoporotic women. Bone. 2005; 36:948–958.15. Beck TJ, Looker AC, Ruff CB, Sievanen H, Wahner HW. Structural trends in the aging femoral neck and proximal shaft: analysis of the Third National Health and Nutrition Examination Survey dual-energy X-ray absorptiometry data. J Bone Miner Res. 2000; 15:2297–2304.16. Beck TJ. Hip structural analysis (HSA) program. Baltimore: Johns Hopkins University;2002.17. Kaptoge S, Beck TJ, Reeve J, Stone KL, Hillier TA, Cauley JA, et al. Prediction of incident hip fracture risk by femur geometry variables measured by hip structural analysis in the study of osteoporotic fractures. J Bone Miner Res. 2008; 23:1892–1904.18. Carter PH, Schipani E. The roles of parathyroid hormone and calcitonin in bone remodeling: prospects for novel therapeutics. Endocr Metab Immune Disord Drug Targets. 2006; 6:59–76.19. Rubin MR, Dempster DW, Zhou H, Shane E, Nickolas T, Sliney J Jr, et al. Dynamic and structural properties of the skeleton in hypoparathyroidism. J Bone Miner Res. 2008; 23:2018–2024.20. Chen Q, Kaji H, Iu MF, Nomura R, Sowa H, Yamauchi M, et al. Effects of an excess and a deficiency of endogenous parathyroid hormone on volumetric bone mineral density and bone geometry determined by peripheral quantitative computed tomography in female subjects. J Clin Endocrinol Metab. 2003; 88:4655–4658.21. Szulc P, Duboeuf F, Schott AM, Dargent-Molina P, Meunier PJ, Delmas PD. Structural determinants of hip fracture in elderly women: re-analysis of the data from the EPIDOS study. Osteoporos Int. 2006; 17:231–236.22. Schaadt O, Bohr H. Different trends of age-related diminution of bone mineral content in the lumbar spine, femoral neck, and femoral shaft in women. Calcif Tissue Int. 1988; 42:71–76.23. Bohr H, Schaadt O. Bone mineral content of the femoral neck and shaft: relation between cortical and trabecular bone. Calcif Tissue Int. 1985; 37:340–344.24. Kricun ME. Red-yellow marrow conversion: its effect on the location of some solitary bone lesions. Skeletal Radiol. 1985; 14:10–19.25. Ominsky MS, Libanati C, Niu QT, Boyce RW, Kostenuik PJ, Wagman RB, et al. Sustained modeling-based bone formation during adulthood in cynomolgus monkeys may contribute to continuous BMD gains with denosumab. J Bone Miner Res. 2015; 30:1280–1289.26. Beck TJ. Extending DXA beyond bone mineral density: understanding hip structure analysis. Curr Osteoporos Rep. 2007; 5:49–55.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Type 2 diabetes mellitus and bone fragility: Special focus on bone imaging
- The Influence of the Left Ventricular Geometry on the Left Atrial Size and Left Ventricular Filling Pressure in Hypertensive Patients, as Assessed by Echocardiography
- Differences in Osteoconduction at Porous Hydroxyapatite according to Pore Geometry
- Effect of Hindlimb Unloading of the Mechanical Properties of Bone in Mature Adult Male Rats: with Emphasis on the Bone Strength
- Titanium Mesh for Bone Augmentation in Oral Implant Surgery
