Recurrence of a Unicameral Bone Cyst in the Femoral Diaphysis
- Affiliations
-
- 1Department of Orthopedic Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jss3505@skku.edu
- KMID: 2412334
- DOI: http://doi.org/10.4055/cios.2016.8.4.484
Abstract
- Diaphyseal unicameral bone cysts of the long bone are generally known to originate near the growth plate and migrate from the metaphysis to the diaphysis during skeletal growth. In the case of unicameral bone cysts of diaphyseal origin, recurrence at the same location is extremely rare. We report a case of recurrence of a unicameral bone cyst in the diaphysis of the femur that developed 8 years after treatment with curettage and bone grafting. We performed bone grafting and lengthening of the affected femur with an application of the Ilizarov apparatus over an intramedullary nail to treat the cystic lesion and limb length discrepancy simultaneously.
Keyword
MeSH Terms
Figure
-
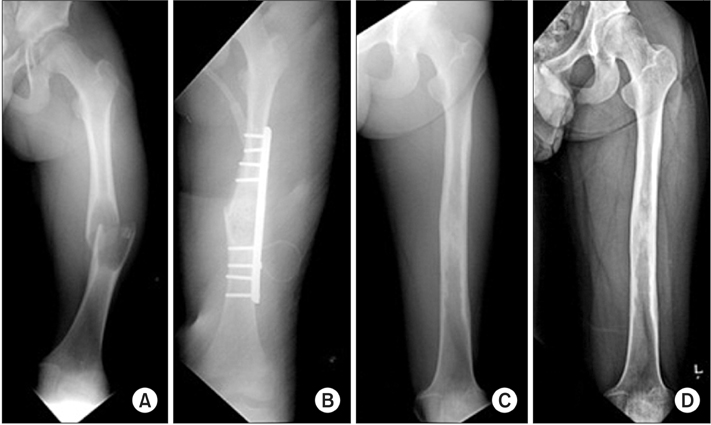
Fig. 1 (A) Initial plain radiograph showing a concentric osteolytic lesion with cortical thinning and ballooning in the mid-portion of the femur shaft accompanied by a pathologic fracture. (B) Radiograph taken after curettage of the cystic lesion and bone grafting followed by open reduction and internal fixation for the pathologic fracture. (C) Two-year follow-up radiograph showing complete healing of the cystic bone lesion. (D) Seven-year follow-up radiograph showing no recurrence of the cyst in the femur.
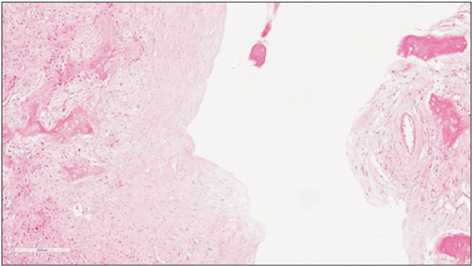
Fig. 2 Lining of the simple bone cyst composed of fibrous tissue without obvious lining cells (H&E, × 50).

Fig. 3 Long bone scanogram obtained at skeletal maturity showing a leg length discrepancy of 3.5 cm.

Fig. 4 (A) Eight-year follow-up radiograph showing an impending pathologic fracture caused by a recurrent simple bone cyst in the left femur. (B) Magnetic resonance imaging scan demonstrating a 6.6 cm × 3 cm × 3 cm-sized, well-defined cystic lesion in the left distal femur. (C) Radiograph taken after curettage and autogenous bone grafting combined with internal fixation using an intramedullary nail.

Fig. 5 (A) Radiograph taken 1 year after the second surgery showing stability of the lesion despite cortical thinning and ballooning of the femur. (B) Radiograph taken after lengthening of the left femur with an application of the Ilizarov apparatus over the intramedullary nail. (C) Radiograph taken 20 months after distraction osteogenesis showing no evidence of recurrence.
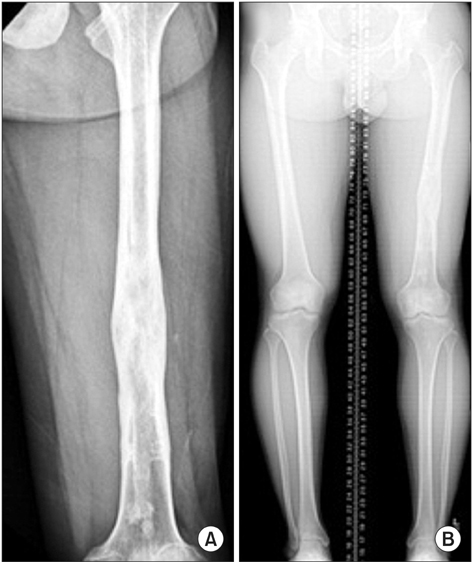
Fig. 6 (A) Radiograph taken after hardware removal at 30 months after the distraction osteogenesis. (B) Long bone scanogram obtained at skeletal maturity showing no limb length discrepancy.
Reference
-
1. Lokiec F, Wientroub S. Simple bone cyst: etiology, classification, pathology, and treatment modalities. J Pediatr Orthop B. 1998; 7(4):262–273.2. Cohen J. Etiology of simple bone cyst. J Bone Joint Surg Am. 1970; 52(7):1493–1497.
Article3. Jaffe HL, Lichtenstein L. Solitary unicameral bone cyst with emphasis on the roentgen picture, the pathologic appearance and the pathogenesis. Arch Surg. 1942; 44(6):1004–1025.4. Watanabe H, Arita S, Chigira M. Aetiology of a simple bone cyst: a case report. Int Orthop. 1994; 18(1):16–19.5. Helms CA. Fundamentals of skeletal radiology. 2nd ed. Philadelphia, PA: Elsevier Saunders;1995.6. Bowen RE, Morrissy RT. Recurrence of a unicameral bone cyst in the proximal part of the fibula after en bloc resection: a case report. J Bone Joint Surg Am. 2004; 86(1):154–158.
Article7. Tsuchiya H, Morsy AF, Matsubara H, Watanabe K, Abdel-Wanis ME, Tomita K. Treatment of benign bone tumours using external fixation. J Bone Joint Surg Br. 2007; 89(8):1077–1083.
Article8. Jesus-Garcia R, Bongiovanni JC, Korukian M, Boatto H, Seixas MT, Laredo J. Use of the Ilizarov external fixator in the treatment of patients with Ollier's disease. Clin Orthop Relat Res. 2001; (382):82–86.
Article9. Violas P, Salmeron F, Chapuis M, Sales de Gauzy J, Bracq H, Cahuzac JP. Simple bone cysts of the proximal humerus complicated with growth arrest. Acta Orthop Belg. 2004; 70(2):166–170.10. Glowacki M, Ignys-O'Byrne A, Ignys I, Wroblewska K. Limb shortening in the course of solitary bone cyst treatment: a comparative study. Skeletal Radiol. 2011; 40(2):173–179.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Unicameral Bone Cyst with Fracture of Femoral Neck
- Unicameral Bone Cyst
- The Treatment of Unicameral Bone Cysts by Topical Injection of Methylprednisolone Acetate: Reaport of 4 Cases
- Intramedullary Decompression for the Treatment of Unicameral Bone Cysts in Children
- The treatment of unicameral bone cyst by topical injection of methylprednisolone acetate
