Full mouth rehabilitation of the elderly patient on anticoagulant medication with loss of vertical dimension due to severely worn dentition
- Affiliations
-
- 1Department of Prosthodontics, School of Dentistry, Seoul National University, Seoul, Republic of Korea. young21c@snu.ac.kr
- KMID: 2402988
- DOI: http://doi.org/10.4047/jkap.2018.56.1.56
Abstract
- Severe dental attrition causes pathological changes of the tooth, collapsed occlusion, and functional and aesthetic complications and can also result in a decrease in occlusal vertical dimension. Before increasing the vertical dimension with full-mouth rehabilitation, it is important to determine the amount of vertical dimension through accurate diagnosis. In this case, a 77 year old elderly male patient on anticoagulant medication with generalized attrition and fracture of teeth was treated with full-mouth rehabilitation in order to recover vertical dimension and aesthetics. Accurate clinical and radiographic examination, diagnostic, wax-up, and occlusal vertical dimension evaluation were step by step performed considering pre-medical history and old age. Patient adaptability was evaluated using an occlusal splint and interim restoration. After 3 months of stabilization with interim restoration, definitive prostheses were fabricated. Satisfactory functional and esthetic outcomes are observed after 6 months of follow up.
MeSH Terms
Figure
-

Fig. 1 Intraoral photograph before treatment. (A) Maxillary, (B) Right, (C) Frontal, (D) Left, (E) Mandibular.
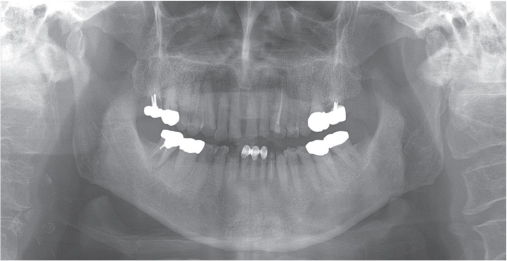
Fig. 2 Panoramic radiograph before treatment.

Fig. 3 Occlusal splint with an increase of vertical dimension.

Fig. 4 Diagnostic wax up model.

Fig. 5 Provisional restoration.
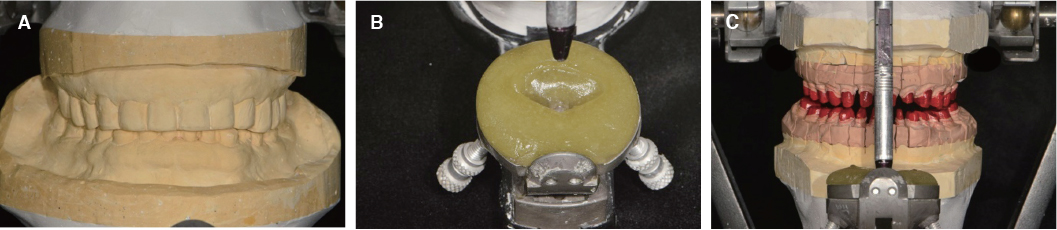
Fig. 6 Cross articulation. (A) Mounting of provisional restoration, (B) Customized guide table, (C) Mounting of working cast.
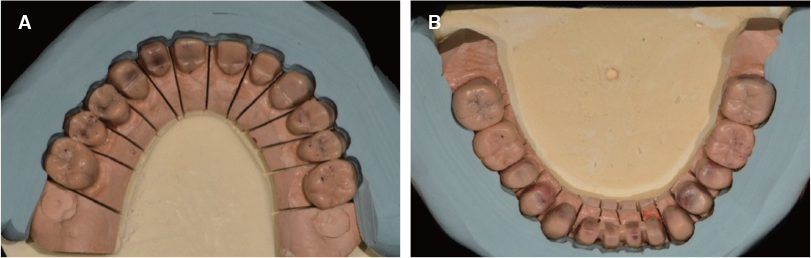
Fig. 7 Full contour wax up cut back. (A) Maxilla, (B) Mandible.

Fig. 8 (A) Metal coping try-in, (B) Porcelain build up before glazing.

Fig. 9 Clinical remounting procedure. (A) Maxillary pick-up impression, (B) Mandibular pick-up impression, (C) Remounting.

Fig. 10 Definitive prosthesis. (A) Maxillary, (B) Right, (C) Frontal, (D) Left, (E) Mandibular.

Fig. 11 Panoramic radiograph after treatment.

Fig. 12 TMJ Panoramic view after treatment. (A) Right opening, (B) Left opening.
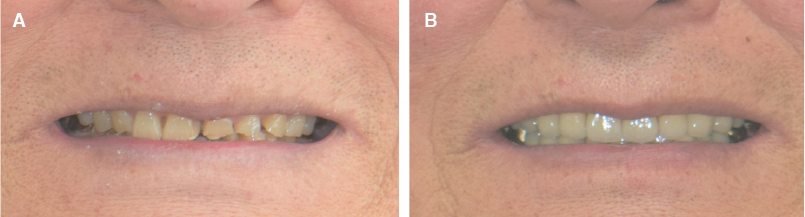
Fig. 13 Comparision image before (A) and after (B) treatment.
Reference
-
1. Dawson PE. Functional Occlusion: from TMJ to smile design. St. Louis; MO: Mosby;2007. p. 430–452.2. Lerner J. A systematic approach to full-mouth reconstruction of the severely worn dentition. Pract Proced Aesthet Dent. 2008; 20:81–87.3. Dombrady L. Investigation into the transient instability of the rest position. J Prosthet Dent. 1966; 16:479–490.
Article4. Tallgren A, Lang BR, Walker GF, Ash MM Jr. Changes in jaw relations, hyoid position, and head posture in complete denture wearers. J Prosthet Dent. 1983; 50:148–156.
Article5. Murphy T. Compensatory mechanisms in facial height adjustment to functional tooth attrition. Australian Dent J. 1959; 4:312–323.
Article6. Berry DC, Poole DF. Attrition: possible mechanisms of compensation. J Oral Rehabil. 1976; 3:201–206.
Article7. Rivera-Morales WC, Mohl ND. Restoration of the vertical dimension of occlusion in the severely worn dentition. Dent Clin North Am. 1992; 36:651–664.8. Turner KA, Missirlian DM. Restoration of the extremely worn dentition. J Prosthet Dent. 1984; 52:467–474.
Article9. McGEE GF. Use of facial measurements in determining vertical dimension. J Am Dent Assoc. 1947; 35:342–350.
Article10. Willis FM. Features of the face involved in full denture prosthesis. Dent Cosmos. 1935; 77:851–854.11. Oh SC, Jung JH. Morphology and size of clinical crown of permanent upper anterior teeth in Korean adult. J Korean Acad Stomatognathic Funct Occlusion. 2001; 17:37–42.12. Kwon KR. The prosthetic approach for collapsed vertical dimensions of occlusion. J Dent Rehabil Appl Sci. 2004; 20:169–181.13. Nelson SJ. Wheeler's dental anatomy, physiology and occlusion. 9th ed. St. Louis: Sanunders Elsevier Health Sciences;2009. p. 99–139.14. Grippo JO, Simring M, Schreiner S. Attrition, abrasion, corrosion and abfraction revisited: a new perspective on tooth surface lesions. J Am Dent Assoc. 2004; 135:1109–1118.15. Ahmad I. Geometric considerations in anterior dental aesthetics: restorative principles. Pract Periodontics Aesthet Dent. 1998; 10:813–822.16. Wood GN. Centric relation and the treatment position in rehabilitating occlusions: a physiologic approach. Part II: The treatment position. J Prosthet Dent. 1988; 60:15–18.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Full-mouth rehabilitation with increasing minimum vertical dimension in the patient with severely worn dentition and deep bite
- Full mouth rehabilitation of a patient with worn dentition and loss of posterior support by vertical dimension reestablishment: a clinical report
- Full mouth rehabilitation with extremely worn dentition
- Full mouth rehabilitation of patient with decreased occlusal vertical dimension due to severely worn dentition and posterior bite collapse
- Complete mouth rehabilitation with vertical dimension increase in patient with extremely worn dentition
