The Incidence of Riata Defibrillator Lead Failure: a Single-Center Experience
- Affiliations
-
- 1Division of Cardiology, Department of Internal Medicine, Heart Vascular Stroke Institute, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. js58.kim@samsung.com
- KMID: 2400432
- DOI: http://doi.org/10.3346/jkms.2017.32.10.1610
Abstract
- Riata defibrillator leads were recalled due to a high failure rate. This study measured the incidence of externalized conductor (EC) and electrical dysfunction (ED) and sought to determine the predictors of ED with Riata defibrillator leads. We enrolled patients who received Riata® or Riata® ST silicone defibrillator leads at our center between January 2003 and December 2010. The presence of EC was evaluated with chest radiography. The incidence rates were measured at < 3 years, 3-5 years, and > 5 years after lead implantation. We also investigated the rates of ED and other clinical events during the follow-up period. A total of 44 patients were analyzed. The total cumulative incidence of EC was 27.3%. During the median dwell time (80 months), the incidence of ED was 22.7%. Patients with ED were younger (46.5 vs. 56.5 years, P = 0.018) and had a higher prevalence of cardiomyopathy than those without ED (60.0% vs. 20.6%, P = 0.043). ECs were most frequently detected in patients who underwent X-ray analysis 3-5 years after lead implantation (44.4%). In contrast, ED had a bimodal incidence pattern, with peaks at 5 years (7.0%) and 9 years (5.3%). There was no difference in ED-free survival rate between patients with and without EC (P = 0.628). Given the delayed occurrence of EC and ED after implantation of Riata defibrillator leads, long-term close monitoring is critically important.
MeSH Terms
Figure
-
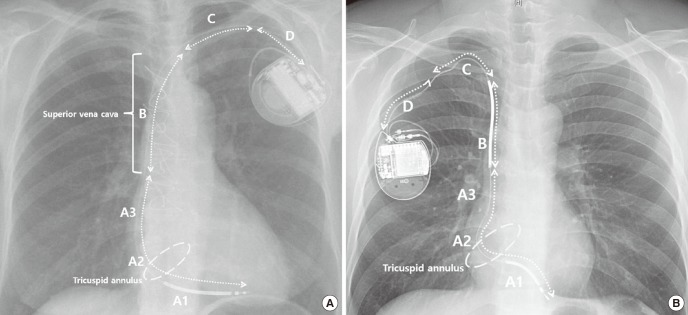
Fig. 1 Location of conductor externalization on chest X-ray (posterior-anterior view). (A) Single coil lead. (B) Dual coil lead.A = distal to the SVC coil (dual coil lead) or distal to the SVC (single coil lead) (A1, proximal right ventricular coil to the tricuspid annulus; A2, tricuspid annulus; A3, tricuspid annulus to the SVC coil [dual coil lead] or right atrium [single coil lead]), B = distal to the clavicle including the SVC coil (dual coil lead) or SVC area (single coil lead), C = clavicular area, D = distal clavicle to the generator can, SVC = superior vena cava.
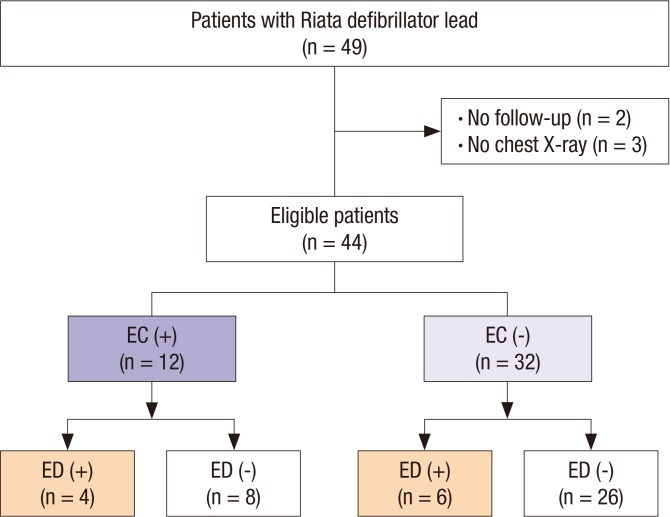
Fig. 2 Flow diagram of study patients.EC = externalized conductor, ED = electrical dysfunction.
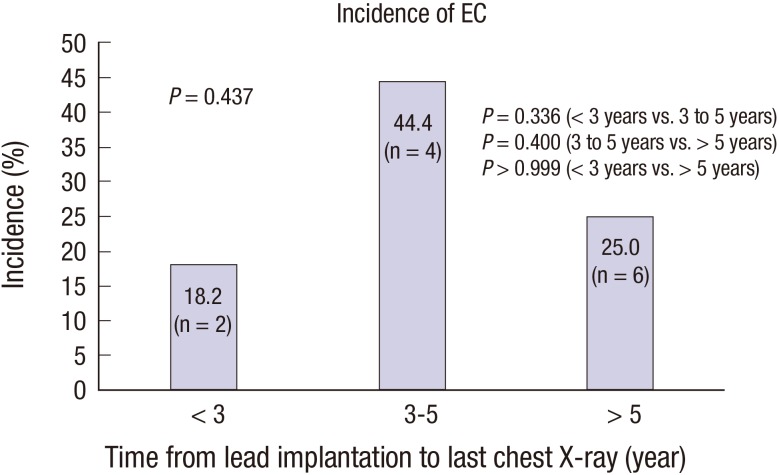
Fig. 3 Incidence of EC of Riata leads on follow-up chest X-ray.EC = externalized conductor.
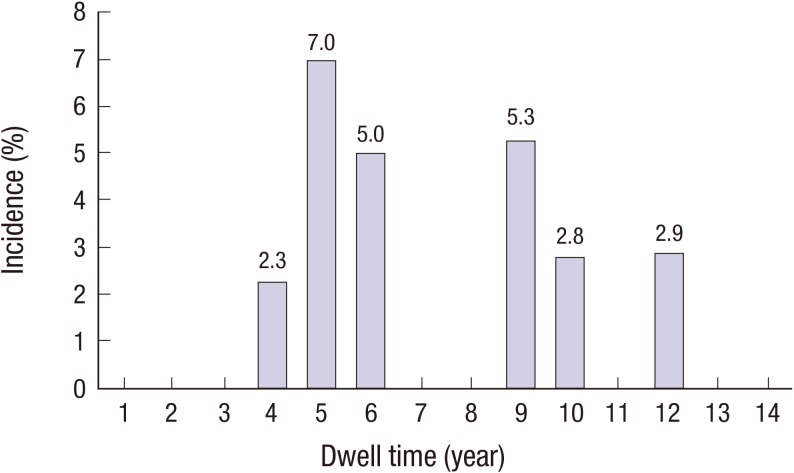
Fig. 4 The incidence of ED according to dwell time.ED = electrical dysfunction.
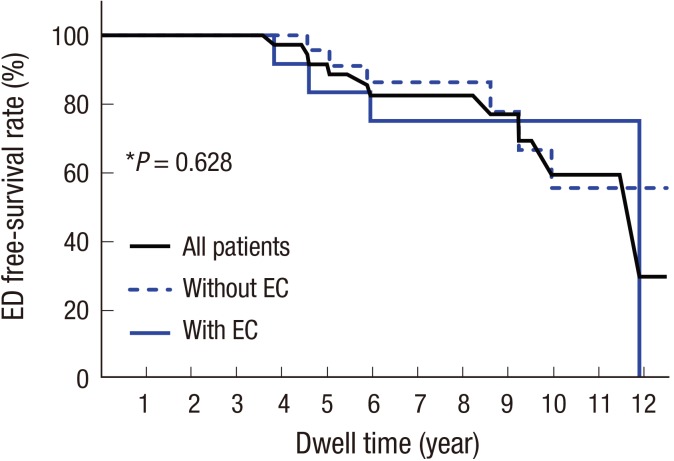
Fig. 5 Kaplan-Meier curve of cumulative probabilities of ED-free survival according to the EC of Riata leads.*P value refers to the result of the log-rank test between patients with and without ECs.EC = externalized conductor, ED = electrical dysfunction.
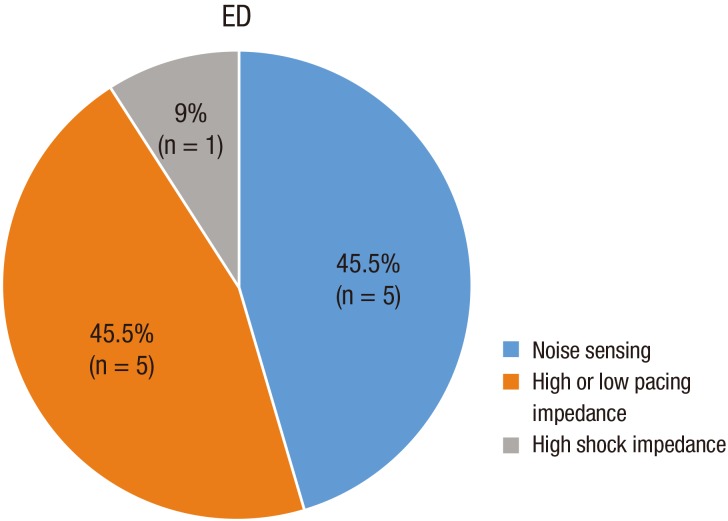
Fig. 6 Different types of electrical lead dysfunction.ED = electrical dysfunction.
Reference
-
1. Zipes DP, Wellens HJ. Sudden cardiac death. Circulation. 1998; 98:2334–2351. PMID: 9826323.2. Kuck KH, Cappato R, Siebels J, Rüppel R. Randomized comparison of antiarrhythmic drug therapy with implantable defibrillators in patients resuscitated from cardiac arrest: the Cardiac Arrest Study Hamburg (CASH). Circulation. 2000; 102:748–754. PMID: 10942742.3. Antiarrhythmics versus Implantable Defibrillators (AVID) Investigators. A comparison of antiarrhythmic-drug therapy with implantable defibrillators in patients resuscitated from near-fatal ventricular arrhythmias. N Engl J Med. 1997; 337:1576–1583. PMID: 9411221.4. Liu J, Rattan R, Adelstein E, Barrington W, Bazaz R, Brode S, Jain S, Mendenhall GS, Nemec J, Razak E, et al. Fluoroscopic screening of asymptomatic patients implanted with the recalled Riata lead family. Circ Arrhythm Electrophysiol. 2012; 5:809–814. PMID: 22787015.5. Larsen JM, Nielsen JC, Johansen JB, Haarbo J, Petersen HH, Thøgersen AM, Hjortshøj SP. Prospective nationwide fluoroscopic and electrical longitudinal follow-up of recalled Riata defibrillator leads in Denmark. Heart Rhythm. 2014; 11:2141–2147. PMID: 25008285.6. Demirel F, Adiyaman A, Delnoy PP, Smit JJ, Ramdat Misier AR, Elvan A. Mechanical and electrical dysfunction of Riata implantable cardioverter-defibrillator leads. Europace. 2014; 16:1787–1794. PMID: 24843049.7. Larsen JM, Riahi S, Nielsen JC, Videbaek R, Haarbo J, Due KM, Theuns DA, Johansen JB. Nationwide fluoroscopic screening of recalled Riata defibrillator leads in Denmark. Heart Rhythm. 2013; 10:821–827. PMID: 23416377.8. Richardson TD, Kolek MJ, Goyal SK, Shoemaker MB, Lewis AA, Rottman JN, Whalen SP, Ellis CR. Comparative outcomes of transvenous extraction of sprint fidelis and Riata defibrillator leads: a single center experience. J Cardiovasc Electrophysiol. 2014; 25:36–42. PMID: 24028661.9. Bongiorni MG, Di Cori A, Segreti L, Zucchelli G, Viani S, Paperini L, De Lucia R, Levorato D, Boem A, Soldati E. Transvenous extraction profile of Riata leads: procedural outcomes and technical complexity of mechanical removal. Heart Rhythm. 2015; 12:580–587. PMID: 25499627.10. Choi K, Kim JH, Kim HJ, Lee SO, Jang EY, Kim JS. A case of riata® dual coil defibrillator lead failure in a patient with ventricular fibrillation. Korean Circ J. 2013; 43:336–339. PMID: 23755080.11. Hayes D, Freedman R, Curtis AB, Niebauer M, Neal Kay G, Dinerman J, Beau S. Prevalence of externalized conductors in Riata and Riata ST silicone leads: results from the prospective, multicenter Riata Lead Evaluation Study. Heart Rhythm. 2013; 10:1778–1782. PMID: 23994078.12. Theuns DA, Elvan A, de Voogt W, de Cock CC, van Erven L, Meine M. Prevalence and presentation of externalized conductors and electrical abnormalities in Riata defibrillator leads after fluoroscopic screening: report from the Netherlands Heart Rhythm Association Device Advisory Committee. Circ Arrhythm Electrophysiol. 2012; 5:1059–1063. PMID: 23091049.13. Duray GZ, Israel CW, Schmitt J, Hohnloser SH. Implantable cardioverter-defibrillator lead disintegration at the level of the tricuspid valve. Heart Rhythm. 2008; 5:1224–1225. PMID: 18675238.14. Steinberg C, Sarrazin JF, Philippon F, Bouchard MA, O'Hara G, Molin F, Nault I, Blier L, Champagne J. Detection of high incidence of Riata lead breaches by systematic postero-anterior and lateral chest X-ray in a large cohort. Europace. 2013; 15:402–408. PMID: 23118004.15. El-Chami MF, Merchant FM, Levy M, Alam MB, Rattan R, Hoskins MH, Langberg JJ, Delurgio D, Lloyd MS, Leon AR, et al. Outcomes of sprint fidelis and Riata lead extraction: data from 2 high-volume centers. Heart Rhythm. 2015; 12:1216–1220. PMID: 25998138.16. Brunner MP, Cronin EM, Jacob J, Duarte VE, Tarakji KG, Martin DO, Callahan T, Borek PP, Cantillon DJ, Niebauer MJ, et al. Transvenous extraction of implantable cardioverter-defibrillator leads under advisory--a comparison of Riata, Sprint Fidelis, and non-recalled implantable cardioverter-defibrillator leads. Heart Rhythm. 2013; 10:1444–1450. PMID: 23816440.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Riata(R) Dual Coil Defibrillator Lead Failure in a Patient with Ventricular Fibrillation
- Delayed Perforation of the Right Ventricular Wall by a Single Standard-Caliber Implantable Cardioverter-Defibrillator Lead Detected by Multidetector Computed Tomography
- Implantable Cardioverter-Defibrillator Lead Extraction by Conventional Traction and Counter-Traction Technique
- Knowledge and Performance Ability of Defibrillator among General Hospital Nurses
- Implantable Cardioverter-Defibrillator Lead Extraction by Conventional Traction and Counter-Traction Technique
